Clinical Efficacy of the Integrative Use of Jiaying Su (Ensure) and Rui Dai (TPF-D) Intestinal Nutrition Formula in ICU Critically Ill Patients
Fei Liu1, Liqian Zhang1, Naikun Gao1, Zhifei Qiao1, Jie Yao2*
1Intensive Care Medicine, The First Affiliated Hospital of Hebei North University, Zhangjiakou, Hebei Province, China
2Anesthesiology Department, The First Affiliated Hospital of Hebei North University, Zhangjiakou, Hebei Province, China
*Correspondence to: Jie Yao, Anesthesiology Department, The First Affiliated Hospital of Hebei North University, Changqing Road, Qiaoxi District, Zhangjiakou, 075061, Hebei Province, China; Email: Jingjie1229@163.com
Abstract
Objective: This study aimed to assess the clinical effectiveness of combining Jiaying Su (Ensure) and Rui Dai intestinal nutrition formula (TPF-D) in Intensive Care Unit (ICU) critically ill patients.
Methods: A retrospective analysis was conducted on 79 patients admitted to the ICU ward between January 2022 and January 2024, who received nutritional support therapy. Patients were divided into a control group (receiving Jiaying Su alone) and an observation group (receiving combined Jiaying Su and Rui Dai). Nutritional indicators, blood glucose levels, immune function markers, inflammatory factors, occurrence of complications, and prognosis were compared between the two groups.
Results: After 7 days of treatment, the observation group exhibited a greater increase in serum albumin (ALB) and prealbumin (PAB) levels compared to the control group (P<0.05). Blood glucose levels, including fasting blood glucose (FBG) and postprandial 2-hour postprandial blood glucose, were significantly lower in the observation group than in the control group after treatment (P<0.05). The observation group also demonstrated higher levels of immunoglobulin G, immunoglobulin A, and complement C3 compared to the control group (P<0.05). Inflammatory markers, procalcitonin, and C-reactive protein levels were significantly reduced in both groups after treatment, with greater reductions observed in the observation group (P<0.05). The incidence of enteral nutrition complications was lower in the observation group (P<0.05), while the transfer from ICU to a general ward was higher (P<0.05).
Conclusion: The combined use of Jiaying Su and TPF-D demonstrated favorable clinical efficacy in ICU critically ill patients. Compared to Jiaying Su alone, the addition of Rui Dai promoted better nutritional recovery, regulated blood glucose levels, improved immune function, mitigated inflammatory responses, and enhanced patient prognosis.
Keywords: ICU critically ill patients, Jiaying Su, Rui Dai, intestinal nutrition formula, clinical efficacy
1 INTRODUCTION
Critically ill patients in the intensive care unit (ICU) often experience malnutrition and metabolic disorders as a consequence of the severity of their illness and the physiological stress response elicited during treatment[1]. Malnutrition not only adversely affects the physiological functions of the patients and recovery processes but also significantly increases susceptibility to infections and complications, thus profoundly influencing prognosis and survival rates[2]. Consequently, the provision of effective nutritional support therapy for ICU critically ill patients assumes paramount importance[3]. Intestinal nutrition represents a pivotal approach to nutritional support therapy for such patients. By delivering adequate nutritional support via the enteral route, it not only preserves the integrity and functionality of the intestinal mucosa but also enhances nutrient absorption and utilization within the intestines. Moreover, it contributes to the maintenance of a balanced intestinal microbiota, thereby mitigating the risk of infection, augmenting immune function, and improving overall nutritional status[4,5]. Nonetheless, conventional intestinal nutrition formulas are beset by shortcomings, including inadequate and imbalanced nutritional composition, as well as a proclivity to induce gastrointestinal discomfort, thereby impeding their efficacy and clinical applicability[6-8].
Jiaying Su and Rui Dai are two widely used nutritional formulas in recent years for intestinal nutrition therapy. Jiaying Su is a complete nutritional formula with high bioavailability and safety, suitable for various critically ill patients. It is also known as amino-acid-based formula, is suitable for individuals with lactose intolerance, those unable to consume solid food due to trauma, chronic illness, advanced age, postpartum women, pre- and post-operative patients, and individuals requiring restricted diets. It is formulated in proportion to the recommended daily dietary allowances and contains a variety of essential nutrients such as carbohydrates, proteins, fats, vitamins, electrolytes, and trace elements necessary for human bodily functions. Rui Dai is an intestinal nutrition formula containing immunomodulators, glutamine peptides, and other bioactive ingredients, which can enhance intestinal mucosal barrier function, improve immune function, and prevent infections. However, there is limited research on the clinical effects of the combined use of Jiaying Su and Rui Dai in nutritional support therapy for ICU critically ill patients. Therefore, this study aims to retro Rui Dai intestinal nutrition formula (TPF-D) spectively analyze the data of ICU critically ill patients admitted to our hospital over the past two years, evaluate the clinical efficacy of the combined use of Jiaying Su and Rui Dai in nutritional support therapy for critically ill patients, and provide more effective nutritional support therapy strategies for clinical practice to improve the prognosis and quality of life of ICU critically ill patients.
2 DATA AND METHODS
2.1 Study Design
A retrospective analysis was conducted on the clinical data of 79 critically ill patients admitted to the ICU ward of our hospital and receiving nutritional support therapy from January 2022 to January 2024. Inclusion criteria: Patients aged ≥18 years, of any gender; patients with stable hemodynamics, normal intestinal function, Nutritional Risk Screening 2002 (NRS 2002)[9] score ≥3, requiring nutritional support therapy; complete and authentic clinical data available for analysis. Exclusion criteria: Severe organ dysfunction; abnormalities in immune function, coagulation function, hematopoietic function, etc.; presence of malignant tumors, gastrointestinal diseases; severe infections, bleeding tendencies; allergies or relevant contraindications to drugs or methods used in this study; concomitant cognitive impairment, consciousness disorders, and/or mental illnesses. Patients were divided into control (n=39) and observation (n=40) groups based on the enteral nutrition intervention they received. The baseline data of the two groups were comparable (P>0.05), as detailed in Table 1. The present study received ethical approval from the Ethical Committee of The First Affiliated Hospital of Hebei North University (approval No. 29830). The study was conducted in accordance with the ethical guidelines outlined by the committee.
Table 1. Comparison of Basic Information (x±s, n [%])
|
Control (n=39) |
Observation (n=40) |
t/x² |
P |
Gender |
- |
- |
1.031 |
0.309 |
Male |
22 (56.41) |
27 (67.50) |
- |
- |
Female |
17 (43.59) |
13 (32.50) |
- |
- |
Age (years) |
50.83±4.19 |
52.19±4.46 |
1.396 |
0.166 |
Body Mass Index (kg/m²) |
21.56±1.13 |
21.27±1.34 |
1.038 |
0.302 |
NRS 2002 Score |
4.47±0.62 |
4.65±0.71 |
1.199 |
0.234 |
Primary Disease |
- |
- |
0.380 |
0.537 |
Cerebral Hemorrhage |
9 (23.08) |
7 (17.50) |
- |
- |
Cerebral Infarction |
15 (38.46) |
14 (35.00) |
- |
- |
Chronic Obstructive Pulmonary Disease |
6 (15.38) |
7 (17.50) |
- |
- |
Head Trauma |
4 (10.26) |
5 (12.50) |
- |
- |
Severe Pneumonia |
3 (7.69) |
4 (10.00) |
- |
- |
Other |
2 (5.13) |
3 (7.50) |
- |
- |
2.2 Methods
Patients admitted to the hospital were given routine symptomatic supportive treatments including anti-infection and blood glucose control. Different enteral nutrition formulas were selected based on patient groups, and the treatment method (enteral feeding or oral intake) was chosen according to the condition of patients. Enteral nutrition therapy followed the principle of starting with small doses and gradually increasing. The control group received enteral nutrition support therapy with a pure addition of 1,000mL of Jiaying Su (Ensure enteral nutrition powder, with a ratio of 200mL water: 53.8g powder, Abbott Pharmaceutical Co., Ltd., USA). Per 100g of powdered formula, it contains 15.9g of protein, 15.9g of fat, 8.7g of linoleic acid, 61.8g of carbohydrates, and 2.5g of minerals (including 0.36g of sodium, 0.67g of potassium, 0.23g of calcium, 0.23g of phosphorus, 0.61g of chloride, 90mg of magnesium, 4.05mg of iron, 5.1mg of zinc, 0.45mg of copper, 34ug of iodine, and 1.12mg of manganese). It also contains 1130IU of vitamin A, 90IU of vitamin D, 10IU of vitamin E, 116ug of vitamin K, 68mg of vitamin C, 0.68mg of vitamin B1, 0.77mg of vitamin B2, 0.9mg of vitamin B6, 2.7mg of vitamin B12, 9mg of niacin, 9ug of folic acid, 2.3mg of pantothenic acid, 63ug of biotin, and 136mg of choline.
The observation group received enteral nutrition support therapy with a combination of 500mL of Jiaying Su and 500mL of Rui Dai (TPF-D enteral nutrition emulsion, with a ratio of 200mL water: 53.8g powder, F. Hoffmann-La Roche Ltd., Sino-Swiss Pharmaceutical Co., Ltd.). The components include Protein, Carbohydrates, Fat, Vitamin A, Vitamin B1, Vitamin B2, Vitamin B6, Vitamin C, Vitamin D, Vitamin E, Calcium, Iron, Zinc, Selenium, Iodine, Magnesium, Potassium, Sodium, Phosphorus, Chromium, Manganese, Molybdenum, Copper, Fluorine, Choline, Biotin, Niacin, Pantothenic Acid, Folic Acid, and Dietary Fiber. Both groups received continuous treatment for a minimum duration of 7 days, with the infusion rate adjusted according to gastrointestinal condition of each patient (20-80mL/h). Throughout the treatment process, meticulous nutritional records were established for the patients, and personalized nutritional therapy, along with continuous monitoring, was implemented based on individual circumstances. The following measures were undertaken:
2.2.1 Nutritional Assessment
Prior to initiating enteral nutrition support, a comprehensive nutritional assessment was conducted to determine the most suitable formula and develop individualized nutritional treatment plans. The nutritional status of the patients was closely monitored throughout the enteral nutrition support.
2.2.2 Prescription Review
Clinical pharmacists critically reviewed and assessed the rationality of nutritional prescriptions, carefully examining factors such as compatibility contraindications, formula selection, dosage, infusion rate, and feeding route. This process ensured the appropriateness and safety of the prescribed nutrition regimen.
2.2.3 Pharmaceutical Care
Special attention was given to monitoring the gastrointestinal tolerance of patients and addressing any complications associated with the nutritional support therapy. Measures were taken to prevent issues such as feeding tube blockages caused by medication or other factors.
2.3 Observational Indicators
2.3.1 Nutritional Indicator Levels
Before treatment and after 7 days of treatment, 7mL of fasting elbow venous blood was collected from patients in the morning, centrifuged to obtain the supernatant, and serum albumin (ALB), prealbumin (PAB), and hemoglobin (Hb) levels were measured using Beckman Coulter AU680 automatic biochemical analyzer (United States).
2.3.2 Blood Glucose Indicator Levels
Before treatment and after 7 days of treatment, serum specimens were collected from patients (as above), and fasting blood glucose (FBG) and 2-hour postprandial blood glucose (2h BG) levels were measured using an Accu-Chek Active glucose meter (Germany).
2.3.3 Immune Function Indicator Levels
Before treatment and after 7 days of treatment, serum specimens were collected from patients (as above), and levels of immunoglobulin G (IgG), immunoglobulin A (IgA), and complement C3 were measured using a BD FACSCanto flow cytometer (United States).
2.3.4 Inflammatory Factor Indicator Levels
Before treatment and after 7 days of treatment, serum specimens were collected from patients (as above), and levels of procalcitonin (PCT) and C-reactive protein (CRP) were measured using a Roche Cobas c501 automatic biochemical analyzer (Switzerland).
2.3.5 Incidence of Enteral Nutrition Complications and Prognosis
Including gastrointestinal complications (diarrhea, constipation, abdominal distension, nausea, vomiting, etc.), mechanical complications (feeding tube obstruction, difficulty in tube removal, etc.), metabolic abnormalities (electrolyte imbalance, liver function abnormalities, etc.), and infectious complications (aspiration and contamination of nutritional fluids etc.), etc. At the same time, the rate of ICU transfer within 1 month of nutritional support therapy was recorded.
2.3.6 Statistical Analysis
GraphPad Prism 8 software was used for graphical representation, and SPSS 22.0 was used for data analysis. Measurement data were described using (x±s) to represent their distribution and analyzed using t tests; count data were described using n (%) to represent their distribution and analyzed using chi-square tests. P<0.05 indicated statistical significance.
3 RESULTS
3.1 Comparison of Nutritional Indicator Levels
Figure 1 demonstrates that both groups exhibited an increase in ALB and PAB levels after 7 days of treatment, with the observation group displaying a significantly greater change (P<0.05). However, there was no statistically significant difference in Hb levels before and after treatment within either group (P>0.05).
|

Figure 1. Comparison of nutritional indicator levels (x±s, g/L). Compared to before treatment, *P<0.05; intergroup comparison, #P<0.05.
3.2 Comparison of Blood Glucose Indicator Levels
As shown in Figure 2, the observation group experienced a notable decrease in FBG and 2h BG levels after 7 days of treatment compared to both baseline and the control group during the same period (P<0.05).
|
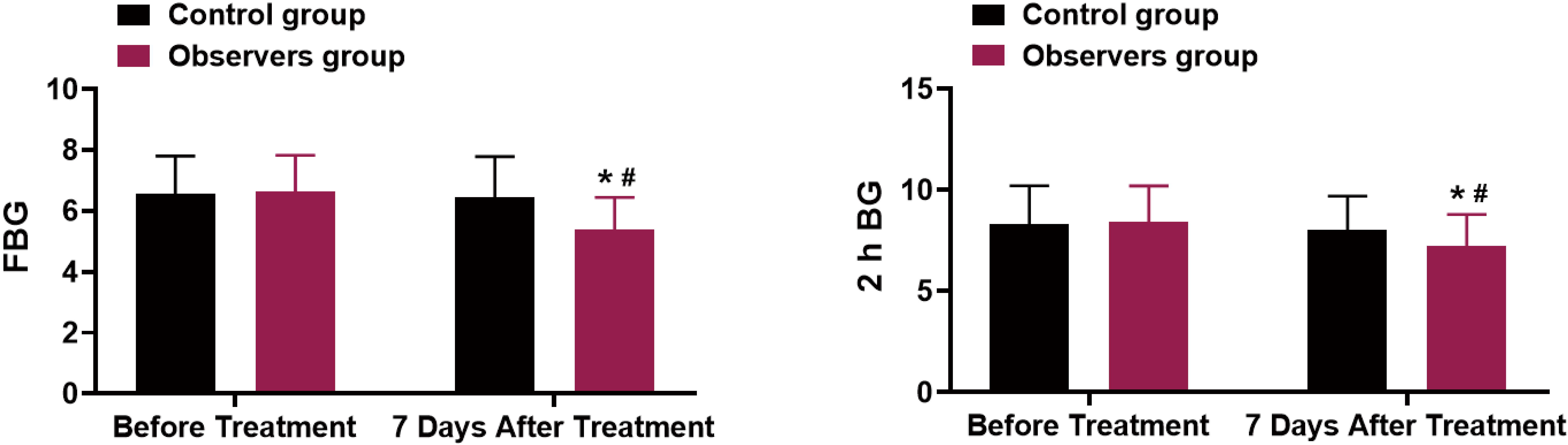
Figure 2. Comparison of Blood Glucose Indicator Levels (x±s, mmol/L). Compared to before treatment, *P<0.05; intergroup comparison, #P<0.05.
3.3 Comparison of Immune Function Indicator Levels
Figure 3 illustrates that the observation group demonstrated a significant increase in IgG, IgA, and complement C3 levels after 7 days of treatment compared to both baseline and the control group (P<0.05). However, there was no statistically significant difference in IgG, IgA, and complement C3 levels before and after treatment in the control group (P>0.05).
|

Figure 3. Comparison of Immune Function Indicator Levels (x±s, g/L). Compared to before treatment, *P<0.05; intergroup comparison, #P<0.05.
3.4 Comparison of Inflammatory Factor Indicator Levels
As depicted in Figure 4, both groups exhibited a decrease in PCT and CRP levels after 7 days of treatment, with the observation group showing a more pronounced change (P<0.05).
|

Figure 4. Comparison of Inflammatory Factor Indicator Levels (x±s). Compared to before treatment, *P<0.05; intergroup comparison, #P<0.05.
3.5 Comparison of Incidence and Prognosis of Complications of Enteral Nutrition
A comparison of the incidence of enteral nutrition complications between the two groups revealed a statistically significant difference (P<0.05). Furthermore, the observation group exhibited a higher rate of ICU transfer compared to the control group (P<0.05), as outlined in Table 2.
Table 2. Incidence and Prognosis of Complications of Enteral Nutrition [n(%)]
Complications |
Control (n=39) |
Observation (n=40) |
x² |
P |
Gastrointestinal Complications |
8 (20.51) |
4 (10.00) |
- |
- |
Mechanical Complications |
1 (2.56) |
2 (5.00) |
- |
- |
Metabolic Abnormalities |
2 (5.13) |
1 (2.50) |
- |
- |
Infectious Complications |
2 (5.13) |
1 (2.50) |
- |
- |
Total Incidence |
13 (33.33) |
8 (20.00) |
1.798 |
0.179 |
ICU Transfer Rate |
14 (35.90) |
28 (70.00) |
9.223 |
0.002 |
4 DISCUSSION
Nutritional support assumes a critical role in the management of ICU critically ill patients, functioning not only as a lifeline but also as a pivotal element in patient resilience against the challenges posed by illness[10,11]. The timely and effective provision of nutritional support holds immense significance, as a failure to do so can directly impact clinical outcomes by depleting the body’s energy and protein reserves, thereby potentially jeopardizing the lives of patients[12]. Within the spectrum of nutritional support, enteral nutrition therapy emerges as a vital modality, delivering essential nutrients and trace elements directly through the gastrointestinal tract and laying the groundwork for all other treatment measures. This therapeutic approach holds the potential to significantly improve nutritional status of patients, bolster immune function, slow disease progression, and contribute to favorable outcomes[13]. Research[14] has demonstrated that, in comparison to traditional parenteral nutrition, enteral nutrition is particularly advantageous in preserving the integrity of the intestinal barrier function, encompassing mechanical, chemical, biological, and immune barriers. Consequently, this therapeutic approach enjoys widespread implementation in clinical practice, particularly in patients necessitating nutritional support, underscoring its paramount importance.
This study compared two different enteral nutrition formulas for ICU critically ill patients, namely, a formula with only Jiaying Su and a formula with Jiaying Su combined with Rui Dai. Various indicators of the patients were evaluated, including nutritional indicators, blood glucose indicators, immune function indicators, levels of inflammatory factors, as well as the impact of enteral nutrition complications and prognosis. The results showed that the enteral nutrition formula combining Jiaying Su and Rui Dai performed better in the nutritional support treatment of ICU critically ill patients. With regards to the nutritional indicators, a statistically significant improvement was observed in the levels of ALB and PAB in both experimental groups following a 7-day treatment protocol. Notably, the observation group exhibited a significantly greater magnitude of change compared to the control group (P<0.05). Conversely, there was no significant alteration in Hb levels between the two groups pre- and post-intervention (P>0.05). These findings substantiate the efficacy of both enteral nutrition formulas in enhancing the nutritional status of patients, with the combined treatment demonstrating a more profound impact. The lack of significant changes in Hb levels may be attributed to the longer erythrocyte generation cycle.
Concerning the blood glucose indicators, the observation group exhibited a substantial decrease in both FBG and 2h BG levels after 7 days of treatment compared to both baseline and the control group during the same timeframe (P<0.05). These findings underscore the superior glycemic regulatory effect of the enteral nutrition formula combining Jiaying Su and Rui Dai. In terms of immune function indicators, the observation group manifested a significant elevation in the levels of IgG, IgA, and complement C3 following a 7-day treatment period in comparison to both baseline and the control group (P<0.05). These outcomes substantiate the immunomodulatory efficacy of the enteral nutrition formula combining Jiaying Su and Rui Dai.
There was no significant difference in IgG, IgA, and complement C3 levels between before and after treatment in the control group (P>0.05), indicating that combined with Rui Dai could improve levels of patients immune function. As for inflammatory factor indicators, the levels of PCT and CRP in both groups decreased after 7 days of treatment, with a greater magnitude of change observed in the observation group (P<0.05), indicating that enteral nutrition support was beneficial in reducing inflammatory response in patients. In terms of prognosis, the ICU discharge rate in the observation group was higher than that in the control group (P<0.05), indicating that the enteral nutrition formula combining Jiaying Su and Rui Dai could further improve prognosis of the patients compared to the formula with only Jiaying Su. The analysis suggests that this improvement may be related to factors such as maintaining good immune function in patients with the combined enteral nutrition formula of Jiaying Su and Rui Dai.
Both Jiaying Su and Rui Dai are different types of enteral nutrition formulas that contain a variety of essential nutrients, including proteins, fats, carbohydrates, vitamins, trace elements, and dietary fiber, which are necessary for improving the nutritional status of ICU critically ill patients[15]. However, their distinct nutrient composition ratios can impact the effectiveness of nutritional support therapy. Rui Dai, as an enteral nutrition emulsion, derives its carbohydrates primarily from cassava starch and cereal starch. This composition helps reduce the glucose load on ICU critically ill patients, stabilize blood sugar levels, and promote blood glucose homeostasis, thereby facilitating improved immune function and reduced inflammation levels[16]. Additionally, Rui Dai is rich in hydrolyzed wheat protein, particularly glutamine peptides (14.4g per 1,000mL of Rui Dai). Glutamine plays a crucial role in enhancing immune function and reducing inflammation. Studies have demonstrated the immune-regulating effects of glutamine, such as its combined treatment with ulinastatin for severe pancreatitis, which effectively reduces inflammation and improves immune levels in patients[17]. Research also suggests the consideration of glutamine supplementation for patients in the recovery phase of severe COVID-19, and the American Society for Parenteral and Enteral Nutrition guidelines recommend adding glutamine to enteral nutrition for ICU patients with burns, extensive trauma, and other conditions[18,19]. Moreover, glutamine participates in the synthesis of glutathione, an important antioxidant, and inhibits the production of pro-inflammatory cytokines, thereby reducing inflammation levels in patients[20]. These studies highlight the crucial role of glutamine in enteral nutrition support therapy, benefiting the recovery of critically ill patients undergoing nutritional support therapy. Furthermore, this study discovered that the combination of Jiaying Su and Rui Dai enteral nutrition formulas yielded greater improvements in immune function and inflammatory response compared to patients receiving only Jiaying Su. The inclusion of Rui Dai, which contains glutamine, may contribute to this enhanced effect.
Complications arising from enteral nutrition support are crucial factors to consider when evaluating the choice of nutritional formulas[21]. In clinical practice, complications associated with enteral nutrition primarily encompass gastrointestinal issues (such as diarrhea, constipation, abdominal distension, nausea, and vomiting), mechanical complications (feeding tube obstruction, difficulties in tube removal), metabolic abnormalities (electrolyte imbalances, abnormal liver function), and infectious complications (aspiration and contamination of nutritional solutions). In this study, gastrointestinal complications were found to be the most common, with diarrhea being the predominant issue in the observation group. This could be attributed to the high dietary fiber content in Rui Dai, which belongs to the isosmotic and fiber-enriched protein category. Dietary fiber possesses a hydrating effect, diluting colonic contents, increasing stool volume, and promoting bowel movements, thereby leading to diarrhea. In contrast, the control group primarily experienced constipation, potentially due to factors such as the absence of dietary fiber. Regarding metabolic abnormalities, the control group primarily exhibited hyperglycemia, whereas no instances of hyperglycemia were observed in the observation group. This finding suggests that the combined use of Rui Dai contributes to effective blood sugar control, possibly owing to the combined effects of cassava starch and cereal starch (which are devoid of lactose) in slowing glucose absorption. This highlights the importance of considering the impact of nutritional formula components on blood sugar regulation in patients with glucose abnormalities. Furthermore, with regard to mechanical and infectious complications observed in both patient groups, the analysis may be attributed to appropriate pharmaceutical interventions and the judicious use of antibiotics.
Collectively, the mechanisms underlying the observed results involve the combined effects of improved nutritional status, enhanced glycemic control, immune-modulating properties of specific components, and reduced inflammatory response. The specific nutrient composition and unique properties of Rui Dai contribute to the superior efficacy of the combined enteral nutrition formula in supporting ICU critically ill nutritional status of patients, immune function, and overall prognosis.
Nutritional indicators: The improvement in nutritional indicators, specifically ALB and PAB levels, can be attributed to the nutrient composition of the enteral nutrition formulas. Both Jiaying Su and Rui Dai contain essential nutrients such as proteins, fats, carbohydrates, vitamins, trace elements, and dietary fiber. These nutrients are necessary for improving the nutritional status of ICU critically ill patients. Adequate protein intake from Jiaying Su and Rui Dai supports the synthesis of albumin and other proteins essential for maintaining proper nutrition. Additionally, the inclusion of Rui Dai in the combined formula may provide specific nutrients that further enhance protein synthesis and nutrient absorption, leading to a more significant improvement in nutritional indicators.
Blood glucose indicators: The combined enteral nutrition formula demonstrated superior glycemic control, as evidenced by significant decreases in FBG and 2h BG levels. Rui Dai, with its composition primarily derived from cassava starch and cereal starch, helps reduce the glucose load on ICU critically ill patients. These starches have a slower rate of glucose release, resulting in more stable blood sugar levels and improved blood glucose homeostasis. The slower absorption of glucose from the combined formula may contribute to better glycemic regulation compared to the formula with Jiaying Su alone.
Immune function indicators: The combined enteral nutrition formula showed a significant elevation in immunoglobulin levels (IgG, IgA) and complement C3, indicating improved immune function. Rui Dai, containing glutamine peptides and other nutrients, plays a crucial role in enhancing immune function. Glutamine, an essential amino acid abundant in Rui Dai, has been shown to regulate immune responses, reduce inflammation, and enhance the body's defense mechanisms. The inclusion of glutamine in the combined formula may contribute to the observed improvements in immune function indicators.
Inflammatory factor indicators: The combined enteral nutrition formula led to a greater reduction in inflammatory markers, including PCT and CRP, compared to the formula with Jiaying Su alone. This reduction in inflammatory response can be attributed to the combined effects of improved nutritional status, adequate protein intake, and specific components of Rui Dai. Glutamine, present in Rui Dai, has been shown to inhibit the production of pro-inflammatory cytokines and reduce inflammation levels in patients. Additionally, the overall improvement in nutritional status from the combined formula may contribute to a reduced inflammatory response.
Prognosis: The higher ICU discharge rate observed in the group receiving the combined formula indicates an improved prognosis. This outcome may be attributed to several factors. Firstly, the combined formula's positive impact on nutritional status, immune function, and inflammatory response may contribute to overall recovery of patients and ability to cope with critical illness. Secondly, the inclusion of Rui Dai, with its unique nutrient composition and potential immunomodulatory effects, may have additional benefits in terms of patient outcomes. The combined formula’s ability to maintain good immune function, reduce inflammation, and support overall recovery may explain the improved prognosis observed in this group.
While this study suggests promising clinical implications for the combined enteral nutrition formula containing Jiaying Su and Rui Dai, it is important to consider the limitations. Single-Center Study: This study was conducted at a single center, which may limit the generalizability of the findings. Further research involving multiple centers and a larger sample size is needed to validate the results and establish broader applicability; Lack of Randomization: The study design did not include randomization of patients into treatment groups. This may introduce potential bias and confounding factors that could influence the results. A randomized controlled trial design would provide stronger evidence to support the findings; Short Follow-up Period: The study had a relatively short follow-up period of 7 days. Longer-term follow-up would provide a more comprehensive understanding of the effects of the combined formula on nutritional status, immune function, and patient outcomes; Potential Confounding Variables: The study did not account for other factors that could impact the results, such as differences in baseline characteristics, concomitant treatments, or variations in individual patient responses. These variables could potentially influence the observed outcomes and should be considered in future studies; Lack of Blinding: The study did not mention whether the researchers and participants were blinded to the treatment groups. Lack of blinding introduces the possibility of bias and may affect the interpretation of the results.
5 CONCLUSION
Compared to enteral nutrition formulas supplemented solely with Jiaying Su, the combination of Jiaying Su and Rui Dai in enteral nutrition formulas demonstrates additional benefits in promoting the recovery of nutritional status, regulating blood sugar levels, enhancing immune function, reducing inflammation response, and improving the prognosis of ICU critically ill patients. However, it is important to acknowledge the limitations of this study. Further research is warranted to confirm the findings and address these limitations to provide more robust evidence for the clinical use of this combined formula in ICU critically ill patients.
Acknowledgements
Not applicable.
Conflicts of Interest
The authors declared no conflict of interest.
Author Contribution
Zhang L, Gao N, Liu F and Yao J equally contributed to concepts, design and definition of intellectual content. In addition, Zhang L, Gao N, Liu F and Yao J were involved in literature search, data collection, data analysis, manuscript preparation, manuscript editing and manuscript review of the article.
Abbreviation List
2h BG, 2-hour postprandial Blood Glucose
ALB, Serum albumin
CRP, C-reactive protein
FBG, Fasting blood glucose
Hb, hemoglobin
ICU, Intensive care unit
IgA, Immunoglobulin A
IgG, Immunoglobulin G
NRS 2002, Nutritional Risk Screening 2002
PAB, Prealbumin
PCT, Procalcitonin
TPF-D, Rui Dai intestinal nutrition formula
References
[1] Mohr N, Wessman B, Bassin B et al. Boarding of critically ill patients in the emergency department. Crit Care Med, 2020; 48: 1180-1187.[DOI]
[2] Perez Ruiz de Garibay A, Kortgen A, Leonhardt J et al. Critical care hepatology: Definitions, incidence, prognosis and role of liver failure in critically ill patients. Crit Care, 2022; 26: 289.[DOI]
[3] Al-Dorzi H, Arabi Y. Nutrition support for critically ill patients. JPEN J Parenter Enteral Nutr, 2021; 45: 47-59.[DOI]
[4] Landais M, Nay M, Auchabie J et al. Continued enteral nutrition until extubation compared with fasting before extubation in patients in the intensive care unit: An open-label, cluster-randomised, parallel-group, non-inferiority trial. Lancet Respir Med, 2023; 11: 319-328.[DOI]
[5] Wang L, Wang Y, Li H et al. Optimizing enteral nutrition delivery by implementing volume-based feeding protocol for critically ill patients: An updated meta-analysis and systematic review. Crit Care, 2023; 27: 173.[DOI]
[6] Hermans A, Laarhuis B, Kouw I et al. Current insights in ICU nutrition: Tailored nutrition. Curr Opin Crit Care, 2023; 29: 101-107.[DOI]
[7] Sinha S, Lath G, Rao S. Safety of enteral nutrition practices: Overcoming the contamination challenges. Indian J Crit Care Med, 2020; 24: 709-712.[DOI]
[8] Premkumar M, Soraisham A, Bagga N et al. Nutritional management of short bowel syndrome. Clin Perinatol, 2022; 49: 557-572.[DOI]
[9] Hersberger L, Bargetzi L, Bargetzi A et al. Nutritional risk screening (NRS 2002) is a strong and modifiable predictor risk score for short-term and long-term clinical outcomes: secondary analysis of a prospective randomised trial. Clin Nutr, 2020; 39: 2720-2729.[DOI]
[10] Pardo E, Lescot T, Preiser J et al. Association between early nutrition support and 28-day mortality in critically ill patients: the FRANS prospective nutrition cohort study. Crit Care, 2023; 27: 7.[DOI]
[11] Alsharif D, Alsharif F, Aljuraiban G et al. Effect of supplemental parenteral nutrition versus enteral nutrition alone on clinical outcomes in critically ill adult patients: A systematic review and meta-analysis of randomized controlled trials. Nutrients, 2020; 12: 2968.[DOI]
[12] Wischmeyer P, Bear D, Berger M et al. Personalized nutrition therapy in critical care: 10 expert recommendations. Crit Care, 2023; 27: 261.[DOI]
[13] Zaragoza-García I, Arias-Rivera S, Frade-Mera M et al. Enteral nutrition management in critically ill adult patients and its relationship with intensive care unit-acquired muscle weakness: A national cohort study. PLoS One, 2023; 18: e0286598.[DOI]
[14] Amano K, Maeda I, Ishiki H et al. Effects of enteral nutrition and parenteral nutrition on survival in patients with advanced cancer cachexia: Analysis of a multicenter prospective cohort study. Clin Nutr, 2021; 40: 1168-1175.[DOI]
[15] Kagan I, Hellerman-Itzhaki M, Bendavid I et al. Controlled enteral nutrition in critical care patients - A randomized clinical trial of a novel management system. Clin Nutr, 2023; 42: 1602-1609.[DOI]
[16] Brito-de la Fuente E, Muñiz-Becerá S, Ascanio G. Lipid emulsions in clinical nutrition: Enteral and parenteral nutrition. Adv Food Nutr Res, 2023; 105: 301-342.[DOI]
[17] Cruzat V, Macedo Rogero M, Noel Keane K et al. Glutamine: Metabolism and immune function, supplementation and clinical translation. Nutrients, 2018; 10: 1564.[DOI]
[18] Martindale R, Patel J, Taylor B et al. Nutrition therapy in critically ill patients with coronavirus disease 2019. JPEN J Parenter Enteral Nutr, 2020; 44: 1174-1184.[DOI]
[19] Compher C, Bingham A, McCall M et al. Guidelines for the provision of nutrition support therapy in the adult critically ill patient: The american society for parenteral and enteral nutrition. JPEN J Parenter Enteral Nutr, 2022; 46: 1458-1459.[DOI]
[20] Yoo H, Yu Y, Sung Y et al. Glutamine reliance in cell metabolism. Exp Mol Med, 2020; 52: 1496-1516.[DOI]
[21] Jordan E, Moore S. Enteral nutrition in critically ill adults: Literature review of protocols. Nurs Crit Care, 2020; 25: 24-30.[DOI]
Copyright © 2024 The Author(s). This open-access article is licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, sharing, adaptation, distribution, and reproduction in any medium, provided the original work is properly cited.


