Factors Contributing to Postoperative Pain in Orthopaedic Surgeries: A Systematic Review
Queen Edward Bohr1, Sabina Gerrard2, Foluke Stella Bosun-Arije3*
1School of Nursing and Midwifery, University of Lancashire, UK
2School of Nursing and Midwifery, University of Central Lancashire, UK
3Department of Nursing, University of Doha for Science and Technology, Doha, Qatar
*Correspondence to: Foluke Stella Bosun-Arije, PhD, University of Doha for Science and Technology, Al Tarafa, Jelaiah Street Duhail North P.O. Box 24449, Doha, Qatar, Email: Folukestella.bosunarije@udst.edu.qa; folukedada2001@yahoo.com
Abstract
Objective: Orthopaedic surgeries are widely performed across the globe. It is pertinent to explore approaches that contribute to alleviating pain, restoring function, and improving the quality of life of patients with musculoskeletal disorders and injuries. The aim of the review was to develop a toolkit, contributing to preoperative assessment to aid clinicians in identifying patients at higher risk of experiencing post-operative (Pre-Op) pain.
Methods: We adopted a systematic review; searched the Cumulative Index to Nursing and Allied Heath Literature (CINAHL), EMBASE, PubMed, Scopus, ScienceDirect, EBSCOhost and ProQuest Central databases for articles published between 2010 and 2024. We adopted a thematic data analysis of the extracted data.
Results: Nine articles were reviewed. Socio-demographic factors, clinical factors and Psychological/behavioural factors were dominant factors contributing to post-orthopaedic surgical pain in patients.
Conclusion: Drawing on the best available evidence, we developed a comprehensive toolkit aimed at improving the understanding and management of post-orthopaedic surgical pain. We recommend piloting this toolkit to evaluate its effectiveness in clinical settings. Central to successful pain alleviation is the integration of pre-surgical and post-surgical pain assessments, which enables more targeted and responsive interventions.
Keywords: postoperative pain; orthopaedic surgeries; pain predictors; pain management
1 INTRODUCTION
Orthopaedic surgeries are conducted globally to improve functionality, for corrective purposes and pain alleviation. The discomfort experienced after surgery can impact not the recovery of the patient but also their mental health, mobility and length of hospital stay[1]. The main objectives of orthopaedic procedures are to alleviate pain, improve functionality and boost the wellbeing of individuals dealing with musculoskeletal conditions and injuries[2]. In the realm of surgery, managing pain remains a significant challenge that poses ongoing issues, for patients and healthcare providers alike[3].
However, with advancements in how surgeries are done and the care provided before and after, a notable number of patients who go through orthopaedic procedures continue to experience moderate to intense pain post-surgery[4]. Intense post-surgical pain could signal the likelihood of lasting pain in the future. Integrative approaches have not been successful mainly because of inconsistent medical protocols and a lack of tailored strategies for managing individual pain levels[5].
A timely identification and evaluation of postoperative pain is more critical to improving patient outcomes[6]. Anticipating pain before surgery is vital as it provides information about each patient’s specific risk factors and allows for the customization of a personalized pain relief strategy[7]. This underscores the importance of gaining a comprehension of the elements that impact post-surgery pain encounters and creating effective solutions to alleviate its effects. The aim of this systematic review is to develop a toolkit for preoperative assessment that can aid clinicians in identifying patients at higher risk of experiencing significant postoperative pain. The Research question posed is: What are contributory factors to higher post-orthopaedic surgical pain?
2 MATERIALS AND METHODS
Two researchers independently searched the Cumulative Index to Nursing and Allied Heath Literature (CINAHL), EMBASE, PubMed, Scopus, ScienceDirect, Google Scholar, EBSCOhost and ProQuest Central databases for articles published between 2010 and 2024. This section encompasses the process of search strategy/data extraction, quality appraisal, data collection and data analysis, processes adopted in this systematic review (Please see Table 1 for the inclusion and exclusion and Table 2 for the search strings).
2.1 Search Strategy
Using various search strategies as truncation, quotation marks, wildcard symbols, keywords, Boolean operator and the patient, intervention and outcome (PIO), a systematic search was conducted across electronic databases over four months (February 2024-June 2024).
2.2 Quality Appraisal
The Critical Appraisal Skills Programme tool to appraise the articles reviewed[8]. All nine articles with a score between 8 and 9 was included in this study. The high score indicates that only articles with high methodological quality is included in this review. This systematic review was reported using the widely recognized four-phase PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) flow diagram which is the standard for reporting systematic reviews (please see Figure 1 for the PRISMA flow diagram).
Table 1. Inclusion and Exclusion Criteria
Inclusion Criteria |
Exclusion Criteria |
Studies on preoperative predictors of post operative pain in orthopaedic surgeries in adults. |
Studies on pediatric orthopaedic surgeries |
Studies published in English language between 2010 and 2024. |
Studies that focused on surgical specialties other than orthopaedics. |
Studies that measure the association between post-op orthopedic pain and at least one preoperative predictor. |
Conference abstract and opinion papers. |
At least a potential predictor is identified preoperatively in the study. |
Surgeries performed under local anesthetics were excluded. |
Table 2. Key Words/ Search Terms/Strings
AND |
Problem |
Intervention |
Outcome |
OR |
Post-op pain |
Orthopaedic surgeries |
Preoperative predictors |
OR |
Post-surgical pain |
Orthopaedic operations |
Preoperative indicators |
OR |
Acute pain |
Knee surgeries |
Preoperative determinants |
OR |
Discomfort |
Hip surgeries |
Preoperative factors |
Ache |
Arthroplasty |
Pain level |
|
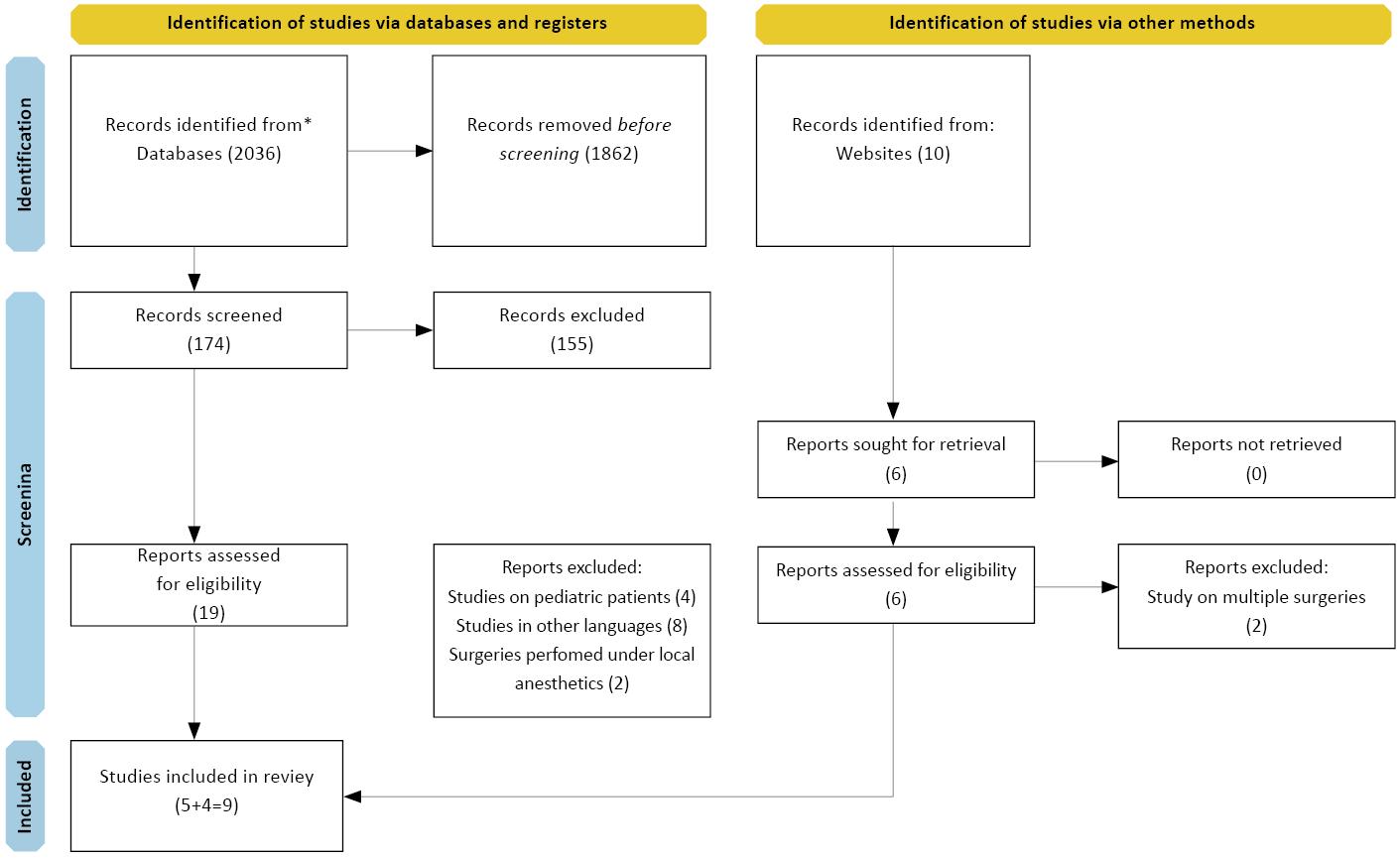
Figure 1. PRISMA Flow Diagram Depicting the Selection Process of Studies for Systematic Review.
We conducted a thematic data analysis of the extracted data. A total of (9) studies were retrieved using the prescribed search strategy which were analyzed for replicability, validity and reliability using various approved critical appraisal tools[8]. See Fig. 1 for the flow diagram of the search process.
For analysis, the nine articles extracted were analysed using the six steps of thematic analysis method40s[9]. In this initial phase of data analysis, the articles were thoroughly read to gain an understanding of the methodologies and findings presented. The goal was to immerse self in the data and obtain a comprehensive overview of the different statistical and analytical techniques used[10]. After the first phase, initial codes were then generated from the summaries of the articles, focusing on predictors and different factors influencing postoperative pain and opioid usage.
Broader themes were subsequently developed to categorize the various methods of analysis from the initial codes[9]. After cross-referencing themes with original articles to ensure they accurately captured the essence of the coded data and resolve discrepancies through reviewing. Three main themes: Sociodemographic predictor of postoperative pain, clinical-related predictors of postoperative pain, psychological and behavioural predictor of postoperative pain were identified, and a summary was produced, detailing the themes identified in the articles.
3 RESULTS
This section entails an overview of the findings. See Table 3 for the summary of the evidence information. Table 4 containing a toolkit that represent the main and minor themes that capture preoperative predictors of post-op pain in orthopaedic surgeries and Tables 5-7 for the recommended aggregate scoring framework.
Table 3. Evidence Table
Author |
Study |
Setting |
Subject |
Surgery |
Result |
[11] |
Prospective observational cohort study. |
Tertiary academic medical center. |
126 patients older than 45 years |
knee replacement at Brigham and Women’s Hospital. |
Revealed several predictors of acute postoperative pain scores including (Temporal summation of pain (TSP); P = 0.001), (Body mass index (BMI); P = 0.044), number of previous knee surgeries (P = 0.006), and female gender (P = 0.023). Similarly, predictors of opioid utilization included TSP (P = 0.011), BMI (P = 0.02), age (P = <0.001), and tourniquet time (P = 0.003). |
[12] |
Multicenter prospective observational study |
Hospital based conducted at two comprehensive specialized hospitals in the PACU, ICU and orthopedic ward |
209 adult patients |
Emergency orthopedic surgeries |
The overall incidence of moderate to severe postoperative pain within the first 24 h after emergency orthopedics surgery was 70.5% (95% CI: 64, 77). On multivariable logistic regression analysis; history of having preoperative pain (Adjusted Odd Ratio (AOR): 7.92, 95% CI: 3.04, 20.63), history of preoperative anxiety (AOR: 6.42, 95% CI: 2.59, 15.90), preoperative patient expectation about postoperative pain (AOR: 6.89, 95% CI: 2.66, 17.78) and being GA (AOR: 4.08, 95% CI: 1.30, 12.77) were significantly associated with moderate to severe postoperative pain after emergency orthopedics surgery. |
[13] |
prospective cohort study |
recuperative pain management service |
97 adult patients |
Primary Total Knee Arthroplasty (TKA) |
After adjusting for all other variables, higher age and catastrophizing pain scores were associated with lower odds of postoperative opioid usage. Increasing age and BMI were associated with lower odds of being referred to pain management. |
[14] |
Prospective study |
Surgeries of Total Hip Arthroplasty (THA) and TKA in the São João Hospital |
95 adult patients |
TKA and THA |
In females, the Acetyl salicylate status 3 physical condition was also associated with higher mean pain intensity. Patients with preoperative chronic pain, without depression diagnosis, and unsatisfied with the current profession showed higher levels of reported pre-operative pain (POP). |
[15] |
SR |
37 articles |
60 years and above |
Knee or hip arthroplasty |
There was a strong association between post-surgical pain and female gender, low socio-economic status, higher pain, comorbidities, low back pain, poor functional status, and depression, anxiety or catastrophic pain. |
[16] |
Pre-operative assessment |
a single urban academic institution |
435 patients |
Various orthopaedic surgery |
435 patients (age=41.1±15.7, 47% female) were studied. Mean PI was 60.1±7.0 prior to surgery and 61.7±7.6 at 2 weeks post-operative (pre-op). Worse 2-week PROMIS PI( A scoring tool used to assess the intensity of pain) was associated with lower extremity surgery, prior surgery on the joint, preoperative opioid use, depression, lower income, lower education, and higher American Society of Anesthesiologists score (P<0.05). |
[17] |
prospective observational study |
in the Post Anesthesia Care Unit. |
153 patients |
Patient who underwent orthopedic surgery procedures |
Preoperative smoking and physical health status were statistically significant predictors of severe postoperative pain in the immediate postoperative period. |
[18] |
Multi-centre, cross sectional, observational study |
Three hospitals for special Surgery (HSS) across America and Canada |
897 patients between ages 18 and 99 |
Total hip or knee replacement |
Predictors for pain at rest were female gender (OR 1.10 with 95 % CI 1.01–1.20), younger age (0.96, 0.94–0.99), increased BMI (1.02, 1.01–1.03), TKR vs. THR (3.21, 2.73–3.78), increased severity of preoperative pain at the surgical site (1.15, 1.03–1.30), preoperative use of opioids (1.63, 1.32–2.01), and GA (8.51, 2.13–33.98). Predictors for pain with activity were TKR vs. THR (1.42, 1.28–1.57), increased severity of POP at the surgical site (1.11, 1.04–1.19), GA (9.02, 3.68–22.07), preoperative use of anti-convulsant (1.78, 1.32–2.40) and anti-depressants (1.50, 1.08–2.80), and prior surgery at the surgical site (1.28, 1.05–1.57). |
[19] |
observational retrospective study |
postoperative care unit (PCU) of a university hospital in Barcelona (Spain) |
127 adult patients |
prosthetic surgery (hip, knee or shoulder arthroplasty |
The prevalence of immediate postoperative pain was 28%. Anxiety was the most common emotional factor (72%) and a predictive risk factor for moderate to severe postoperative pain (OR: 4.60, 95% CI 1.38 to 15.3, P<0.05, AUC: 0.72, 95% CI: 0.62 to 0.83). Age exerted a protective effect (OR 0.96, 95% CI: 0.94-0.99, P<0.01). |
Table 4. The Proposed Pre-op Assessment Toolkit for Post-op Pain
Category |
Sub-category |
Procedure |
Sociodemographic |
Gender |
Document the patient’s gender (Female and Male) |
Age |
Record the patient’s age (18-30 years) (30-45) (≤50) |
|
Race |
Document the patient's race/ethnicity (White, Black or African, Asian, Indigenous and mixed race/multiracial) |
|
BMI |
Calculate BMI (weight in kg/height in m²) BMI Categories: Underweight: <18.5 Normal weight: 18.5-24.9 Overweight: 25-29.9 Obesity: ≥30 |
|
Psychological and bahavioural |
Depression |
Screen for depressive symptoms using standardized tools such as PHQ-9 to assess the severity of depressive symptoms. Score Interpretation: 0-4: Minimal depression 5-9: Mild depression 10-14: Moderate depression 15-19: Moderately severe depression 20-27: Severe depression |
Anxiety |
Assess patients’ anxiety levels using standardized tools such as GAD-7. Score Interpretation: 0-4: Minimal anxiety 5-9: Mild anxiety 10-14: Moderate anxiety 15-21: Severe anxiety |
|
Clinical |
Previous Surgeries |
Document the history of previous surgeries. Assess any complications or chronic pain related to past surgeries. |
Tourniquet Time |
Record the expected tourniquet time for the surgery. |
|
Type of Anaesthetic |
Review the planned type of anesthetic (general, regional, local). |
|
Type of Surgery |
Identify the type of orthopaedic surgery planned. |
|
Preoperative Pain |
Assess preoperative pain levels using tools like Numeric Rating Scale (NRS) or Visual Analog Scale (VAS) NRS/VAS Score Interpretation: 0-3: Mild pain 4-6: Moderate pain 7-10: Severe pain |
|
Table 5. Aggregate Scoring Framework for Sociodemographic Domain (Maximum Score:9)
Variable |
Category |
Score |
Gender |
Male=1, Female=2 (optional if gender-specific risk applies) |
1–2 |
Age |
18–30=1, 31–45=3, ≥50=3 |
1–3 |
Race/Ethnicity |
Black or African=1, White=2, Asian=2, Indigenous=0, Mixed/Multiracial=2 (based on health disparity data) |
0–2 |
BMI Category |
Normal=0, Underweight/Overweight=1, Obese=2 |
0–2 |
Notes: This scoring framework is designed to support risk stratification in health-related assessments, particularly where demographic and anthropometric factors may influence outcomes. Scoring Range: Each variable contributes to a cumulative risk score ranging from 1 to 9. Use Case: This tool may be used to guide tailored interventions, prioritize follow-up, or inform patient education strategies. Equity Consideration: Scores should not be used in isolation to determine care eligibility. They must be interpreted alongside clinical judgment and social determinants of health.
Table 6. Aggregate Scoring Framework for Psychological Domain (Maximum score:48)
Measure |
Tool |
Score Range |
Depression |
PHQ-9 |
10–27 |
Anxiety |
GAD-7 |
10–21 |
Notes: Depression tool: Patient Health Questionnaire-9 (PHQ-9). Scores range from 0-4 to 20–27. Interpretation: For patients scoring in this range of 10-14 and 20-27, it suggests moderate to severe depressive symptoms. Higher scores indicate greater functional impairment and may warrant further evaluation or referral for mental health support. Anxiety tool: Generalized Anxiety Disorder-7 (GAD-7). Scores range from 0-4 to 15–21. Interpretation: For patients scoring in this range of 10-21, it suggests moderate to severe anxiety symptoms. Elevated scores may be associated with persistent worry, somatic complaints, and reduced coping capacity.
Table 7. Aggregate Scoring Framework for Clinical Domain (Maximum score: 8)
Variable |
Category |
Score |
Previous Surgeries |
No=0, Yes=1 |
0–1 |
Tourniquet Time |
<60 min=0, ≥60 min=1 |
0–1 |
Type of Anaesthetic |
Local=0, Regional=1, General=2 |
0–2 |
Type of Surgery |
Minor=0, Moderate=1, Major=2 |
0–2 |
Preoperative Pain |
Mild=0, Moderate=1, Severe=2 |
0–2 |
Notes: Clinical Score=0-8, Higher scores may indicate greater psychosocial burden, surgical complexity, or risk factors. This framework can be adapted for: preoperative risk stratification, educational simulations and patient profiling in research.
3.1 Theme 1: Demographic Predictors of Postoperative Pain
The factors that constitute this theme are gender, age, race, low socio-economic status, and BMI. Out of the nine articles examined, three of them noted that women tend to feel pain than men[11,15,18]. Most of the articles reviewed in this study indicate that younger individuals often mention experiencing post-surgery pain, while advancing age shows a correlation with lower levels of post-surgery pain and reduced use of opioids[15,17-19]. However, there is an argument that African Americans may experience challenges with pain outcomes hinting at potential gaps in how pain is perceived and treated[15].
However other research has shown that there are no association between pain levels and race suggesting that other factors could play a role in shaping this connection[17]. Various articles have discussed the relationship between BMI and postoperative pain with differing conclusions. While some studies highlighted BMI as the predictor, others found multiple factors such as age, gender and race[11,13-15,17,18]. However, there is an affirmation that factors that are significantly correlated with pain, entail age, female gender, BMI, preoperative pain levels, catastrophizing, somatization, average hours of sleep, TSP, and number of previous knee surgeries[11].
3.2 Theme 2: Clinical Predictors of Postoperative Pain
The factors that constitute this theme are linked to previous surgeries, tourniquet time, type of anaesthesia, type of surgery and POP status of patients. Individuals who have undergone procedures, especially those involving the knees are at a higher risk of encountering intense pain following surgery and longer tourniquet times were also associated with greater opioid utilization[11,12,16,18]. Extended periods of application in procedures have been linked to higher levels of pain after surgery, underscoring the importance of adopting meticulous surgical approaches to alleviate postoperative discomfort[11].
The choice of anaesthetic administered during a procedure may impact the amount of pain experienced after the operation. Specifically, regional anaesthesia has been linked to reduced levels of pain when compared to general anaesthesia[12,17,18]. Surgeries on the limbs like knee and hip replacements often result in increased pain after the operation. This highlights the importance of tailored pain management strategies for these procedures[16]. Patients who have pain before surgery tend to have pain after the procedure, highlighting the importance of managing pain before surgery[14,15].
3.3 Theme 3: Psychological and Behavioral Predictors of Postoperative Pain
Apart from smoking, depression and anxiety are the two predominant psychological factors informing this theme. Depression is an important predictor of post-op pain. Individuals experiencing symptoms tend to describe intense pain highlighting the impact of mental wellbeing on how pain is felt and recovery processes after surgery[11,14,16,20].
Three reviewed articles pointed anxiety as a common factor if experienced before surgery, may predict pre-op pain[11,16,19]. Anxiety alleviation through counselling or medication management may relieve a patient of pre-op discomfort.
3.4 Limitations
While this study offers valuable insights into factors contributing to postoperative pain in orthopaedic surgeries, a few limitations must be acknowledged:
(1) Scope and generalisability: Only nine studies were included in this review due to limited literature published on the research topic. Therefore, it is important to note that the limited number of studies included limits the generalisability of the research outcome to a wider population of individuals who have undergone orthopaedic surgeries.
(2) Data collection constraints: Reliance on reviewed articles alone without experts and patients first hand input to the toolkit can potentially introduce biases and the absence of longitudinal data limits the ability to assess sustained impact of the toolkit over time.
The intended use of the toolkit is for clinicians supporting patients who are booked for orthopaedic surgery. The toolkit is developed from the nine practice-based articles reviewed. It was developed through a systematic process of synthesis and translation of the findings of the nine articles reviewed with a goal to transform evidence and insights into practical, user-friendly resources that support implementation, education, or decision-making of clinicians. However, it is important that the proposed toolkit be piloted and refined before disseminated and adopted in clinical settings.
4 DISCUSSION
4.1 Socio-demographic Related Factors as Preoperative Predictors of Postoperative Pain
Some studies report that females are more likely to experience more intense post-op pain compared to males[21,22]. While other studies suggest insignificant variations[23]. The way men and women feel pain differently is thought to be influenced by a mix of hormonal and social factors. There is a significant association between anxiety, current smoking, psychological conditions, and current opioid use with increased preoperative and postoperative reported pain score[23]. Female oestrogen and progesterone are believed to impact how sensitive women are to pain[24]. Younger patients tend to experience pain and the impact of age on pain levels can differs[22,25]. Older individuals may have sensitivity to pain and but are at a higher risk of experiencing complications with opioid based pain management techniques[26]. Different pain perception and analgesic effects among aged groups could be attributed to changes associated with aging[27]. Individuals with high BMI experienced intense pain after surgery and needed a higher amount of pain relief medication right after the operation[22]. While BMI may influence pain perception in some patient populations, it is not a consistent predictor across all surgical contexts[28,29]. It is suggested that when controlling for variables such as socioeconomic factors, healthcare access, and individual health conditions, racial differences in pain perception diminished[30].
4.2 Clinical Related Factors as Preoperative Predictors of Postoperative Pain
Studies have consistently shown that patients with a history of prior surgeries are more likely to experience acute postoperative pain. This phenomenon can be attributed to several factors, including pre-existing pain conditions, altered pain perception, and psychological factors associated with previous surgical experiences. Types of surgeries were also found to have an impact on postoperative pain. Anatomical and physiological changes resulting from previous surgeries can impact pain perception[14]
Prolonged tourniquet times have been linked to increased postoperative pain and other complications. Research highlight that these associations and emphasise the importance of optimal tourniquet management[22,25]. Longer tourniquet times lead to higher levels of postoperative pain and require increased analgesia post-surgery[17]. Similarly, high-pressure inflation and extended duration can lead to muscle and nerve damage, delayed recovery, and increased use of pain medications post-surgery[17]. The choice between anesthesia significantly impacts postoperative pain experiences and outcomes for patients undergoing surgery[31].
4.3 Psychological Related Factors as Preoperative Predictors of Postoperative Pain
Lately, there has been a growing interest in studying the impact of surgery anxiety, on pain levels and recovery after surgery[20]. Confirming the link between surgery anxiety and post-surgery pain is important as it helps identify patients with high anxiety levels beforehand and tailor pain management strategies accordingly[32].
There are discrepancies in how strongly psychosocial factors correlate with surgical outcomes. While anxiety and depression are recognized as significant predictors of postoperative pain, the extent of their impact varies across studies. Some research notes weaker correlations with outcomes like analgesic use or hospital stay length[33,34].
However, psychological factors play a crucial role in postoperative pain perception. Patients with a history of painful surgical experiences may develop anxiety and fear related to new surgical interventions, which can exacerbate their perception of pain. This psychological impact was of previous negative pain impacted the intensity of future surgeries[35]. Addressing anxiety and other psychological factors before surgery can significantly reduce pain levels after the procedure[14].
Depression significantly influences postoperative pain outcomes[14]. Patients experiencing depression often experience a heightened sense of pain intensity due to the emotional and cognitive aspects of depression, which can amplify pain perception[36,37].
The interplay between depression and postoperative pain underscores the need for comprehensive preoperative psychological assessments. Studies suggest that addressing depression preoperatively may enhance overall pain management and improve surgical outcomes. Integrating mental health care into the perioperative process could lead to more effective pain control and better recovery experiences for patients[36,37].
Anxiety is another critical factor that exacerbates postoperative pain. Patients with high levels of psychological factors tend to report more intense pain following surgery[38]. This relationship can be attributed to the physiological and psychological effects of anxiety, which include increased muscle tension, heightened stress responses, and a focus on potential negative outcomes. Anxiety can magnify the perception of pain, making it more challenging for patients to cope with post-op discomfort[39,40].
5 CONCLUSION
Managing post-op pain is crucial for optimising patient outcomes across orthopaedic surgeries. Studies have consistently highlighted diverse factors influencing pain experiences, ranging from demographic, clinical-related and psychological variables are key predictors of pre-op pain. The findings show the importance of tailored pain management protocols with individual risk profiles enhance recovery and improve post-surgical pain management. As a clinical nurse, how would you promote pre and post-surgical pain assessment your practice? How will you identify psychological issues impacting pain management? Reflect and ask yourself if you utilise evidence-based approach to improve pre- and post-surgical pain assessment in your setting?
Acknowledgements
I want to thank my supervisor for her guidance and input into this research.
Conflicts of Interest
The authors declared no conflicts of interest.
Data Availability
All data generated or analysed during this study are included in this published article.
Copyright Permissions
Copyright © 2025 The Author(s). Published by Innovation Forever Publishing Group Limited. This open-access article is licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, sharing, adaptation, distribution, and reproduction in any medium, provided the original work is properly cited.
Author Contribution
Bohr QE contributed to the conceptualisation, methodology, and writing of the original draft. Gerrard S was involved in the conceptualisation, methodology, and review. Bosun-Arije FS oversaw the methodology, conceptualisation, supervision, and the review and editing process.
Abbreviation List
AOR, Adjusted Odd Ratio
BMI, Body Mass Index
NRS, Numeric Rating Scale
POP, pre-operative pain
Pre-Op, Post-operative
THA, Total Hip Arthroplasty
TKA, Total Knee Arthroplasty
TSP, Temporal Summation of Pain
VAS, Visual Analog Scale
References
[1] Sveinsdóttir H, Skúladóttir H. Postoperative psychological distress in patients having total hip or knee replacements: an exploratory panel study. Orthopaedic Nursing, 2012; 31: 302-311.[DOI]
[2] Szeverenyi C, Kekecs Z, Johnson A et al. The use of adjunct psychosocial interventions can decrease postoperative pain and improve the quality of clinical care in orthopedic surgery: a systematic review and meta-analysis of randomized controlled trials. The Journal of Pain, 2018; 19: 1231-1252.[DOI]
[3] Cao W, Ye J, Yan Y et al. General practice management of chronic post-surgical pain in patients with hip fracture: a qualitative study. Frontiers in Medicine, 2024; 10: 1304182.[DOI]
[4] Fuzier R, Rousset J, Bataille B et al. One half of patients reports persistent pain three months after orthopaedic surgery. Anaesthesia Critical Care & Pain Medicine, 2015; 34: 159-164.[DOI]
[5] Schug SA, Palmer GM, Scott DA et al. Acute pain management: scientific evidence, 2015. Medical Journal of Australia, 2016; 204: 315-317.[DOI]https://doi.org/10.5694/mja16.00133
[6] Zhao J. Identifying Distinct Trajectories of Acute Post-Surgical Pain and Their Associations with Persistent Post-Surgical Pain, Opioid Use, and 30-Day Readmission After Abdominal Hysterectomy for Gynecologic Cancer. University of Pittsburgh, 2023.
[7] Vine M, Joseph K, Gibson D et al. Innovative approaches to preoperative care including feasibility, efficacy, and ethical implications: a narrative review. AME Surgical Journal, 2024; 4: 1.[DOI]
[8] Casp UK. CASP checklists. Critical Appraisal Skills Programme (CASP). Oxford, 2018; 33: 121-131.
[9] Braun V, Clarke V. Using thematic analysis in psychology. Qualitative research in psychology, 2006; 3: 77-101.[DOI]
[10] Sivarajah U, Kamal MM, Irani Z et al. Critical analysis of Big Data challenges and analytical methods. Journal of business research, 2017; 70: 263-286.[DOI]
[11] Abrecht CR, Cornelius M, Wu A et al. Prediction of pain and opioid utilization in the perioperative period in patients undergoing primary knee arthroplasty: psychophysical and psychosocial factors. Pain Medicine, 2019; 20: 161-171.[DOI]
[12] Arefayne NR, Tegegne SS, Gebregzi AH et al. Incidence and associated factors of post-operative pain after emergency Orthopedic surgery: A multi-centered prospective observational cohort study. International Journal of Surgery Open, 2020; 27: 103-113.[DOI]
[13] Banka TR, Ruel A, Fields K et al. Preoperative predictors of postoperative opioid usage, pain scores, and referral to a pain management service in total knee arthroplasty. HSS Journal, 2015; 11: 71-75.[DOI]
[14] Gouveia B, Fonseca S, Pozza DH et al. Relationship between postoperative pain and sociocultural level in major orthopedic surgery. Advances in Orthopedics, 2022; 2022: 7867719.[DOI]
[15] Hernández C, Díaz-Heredia J, Berraquero ML et al. Pre-operative predictive factors of post-operative pain in patients with hip or knee arthroplasty: a systematic review. Reumatología Clínica (English Edition), 2015; 11: 361-380.[DOI]
[16] Kator J, Aneizi A, Nadarajah V et al. Predictors of early postoperative pain interference following orthopaedic surgery. Journal of Orthopaedics, 2020; 22: 579-583.[DOI]
[17] Khalil H, Shajrawi A, Henker R. Predictors of severe postoperative pain after orthopedic surgery in the immediate postoperative period. International Journal of Orthopaedic and Trauma Nursing, 2021; 43: 100864.[DOI]
[18] Liu SS, Buvanendran A, Rathmell JP et al. Predictors for moderate to severe acute postoperative pain after total hip and knee replacement. International orthopaedics, 2012; 36: 2261-2267.[DOI]
[19] Robleda G, Sillero-Sillero A, Puig T et al. Influencia del estado emocional prequirúrgico en el dolor postoperatorio tras cirugía ortopédica y traumatológica. Revista Latino-Americana de Enfermagem, 2014; 22: 785-791.[DOI]
[20] Zhang L, Hao LJ, Hou XL et al. Preoperative anxiety and postoperative pain in patients with laparoscopic hysterectomy. Frontiers in psychology, 2021; 12: 727250.[DOI]
[21] Johansen A, Schirmer H, Stubhaug A et al. Persistent post-surgical pain and experimental pain sensitivity in the Tromsø study: comorbid pain matters. PAIN, 2014; 155: 341-348.[DOI]
[22] Nandi M, Schreiber KL, Martel MO et al. Sex differences in negative affect and postoperative pain in patients undergoing total knee arthroplasty. Biology of sex differences, 2019; 10: 23.[DOI]
[23] Armstrong AD, Hassenbein SE, Black S et al. Risk factors for increased postoperative pain and recommended orderset for postoperative analgesic usage. The Clinical journal of pain, 2020; 36: 845-851.[DOI]
[24] Casale R, Atzeni F, Bazzichi L et al. Pain in women: a perspective review on a relevant clinical issue that deserves prioritization. Pain and therapy, 2021; 10: 287-314.[DOI]
[25] Sarhan T, Anwer H. Pectoral Nerve Blocks: Effect Of Addition Of Dexamethasone To Bupivacaine Local Nesthetic On. Pharmacotherapy, 2016; 28: 117-21.
[26] Urban MK, Sasaki M, Schmucker AM et al. Postoperative delirium after major orthopedic surgery. World Journal of Orthopedics, 2020; 11: 90.[DOI]
[27] Jiang Y, Wang Y, Wang R et al. Differences in pain, disability, and psychological function in low back pain patients with and without anxiety. Frontiers in physiology, 2022; 13: 906461
[28] Coppes OJM, Yong RJ, Kaye AD et al. Patient and surgery-related predictors of acute postoperative pain. Current pain and headache reports, 2020; 24: 12.[DOI]
[29] Orhan C, Lenoir D, Favoreel A et al. Culture-sensitive and standard pain neuroscience education improves pain, disability, and pain cognitions in first-generation Turkish migrants with chronic low back pain: a pilot randomized controlled trial. Physiotherapy theory and practice, 2021; 37: 633-645.[DOI]
[30] Thurston KL, Zhang SJ, Wilbanks BA et al. A systematic review of race, sex, and socioeconomic status differences in postoperative pain and pain management. Journal of PeriAnesthesia Nursing, 2023; 38: 504-515.[DOI]
[31] Roh YH, Park SG, Lee S H. Regional versus general anesthesia in postoperative pain management after distal radius fracture surgery: meta-analysis of randomized controlled trials. Journal of Personalized Medicine, 2023; 13: 1543.[DOI]
[32] Ali NN. Assessment of preoperative anxiety, its contributing factors, and impact on immediate postoperative outcomes among cardiac surgery patients-A cross-sectional study. 2023.https://ecommons.aku.edu/theses_dissertations/2169/
[33] Oteri V, Martinelli A, Crivellaro E et al. The impact of preoperative anxiety on patients undergoing brain surgery: a systematic review. Neurosurgical review, 2021; 44: 3047-3057.[DOI]
[34] Salmons HI, Lu Y, Labott JR et al. Identifying modifiable cost drivers of outpatient unicompartmental knee arthroplasty with machine learning. The Journal of Arthroplasty, 2023; 38: 2051-2059. e2.[DOI]
[35] Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. British journal of anaesthesia, 2013; 111: 52-58.[DOI]
[36] Lee S, Xue Y, Petricca J et al. The impact of pre‐operative depression on pain outcomes after major surgery: a systematic review and meta‐analysis. Anaesthesia, 2024; 79: 423-434.[DOI]
[37] Gohari J, Grosman-Rimon L, Arazi M et al. Clinical factors and pre-surgical depression scores predict pain intensity in cardiac surgery patients. BMC anesthesiology, 2022; 22: 204.[DOI]
[38] Costelloe CC, Burns S, Yong RJ et al. An analysis of predictors of persistent postoperative pain in spine surgery. Current pain and headache reports, 2020; 24: 11.[DOI]
[39] Husni M, Jahrami H, Al Shenawi H et al. Postoperative patient pain severity and its association with anxiety, depression, and sleep quality. Cureus, 2024; 16: e54553.[DOI]
[40] Yilmaz Inal F, Yilmaz Camgoz Y, Daskaya H et al. The effect of preoperative anxiety and pain sensitivity on preoperative hemodynamics, propofol consumption, and postoperative recovery and pain in endoscopic ultrasonography. Pain and Therapy, 2021; 10: 1283-1293.[DOI]


