The Impact of Hierarchical Chain Nursing Model on the Resolution Time of Fever and Cough in Children with Pneumonia
Jinying Lu1*, Taotao Chang1, Mingming Hao1, Lijuan Liu1, Zhanru Yin1
1Pediatrics Department, Hengshui People’s Hospital, Hengshui, Hebei Province, China
*Correspondence to: Jinying Lu, Master, Associate professor, Pediatrics Department, Hengshui People’s Hospital, 180 East Renmin Road, 053000, Hengshui, Hebei Province, China; Email: Lujinying0816@163.com
Abstract
Objective: This study investigates the effects of a hierarchical chain nursing model on the resolution time for fever and cough in children diagnosed with pneumonia.
Methods: Eighty children with pneumonia admitted to our hospital between March 2021 and January 2022 were enrolled in this study. The participants were divided into two groups: the observation group and the experimental group, each containing 40 patients, based on the nursing interventions provided. The observation group received standard nursing care, while the experimental group was treated with the hierarchical chain nursing model. We compared clinical outcomes, including the resolution times for symptoms (fever, cough, pulmonary rales), length of hospitalization, pulmonary function indicators [such as peak expiratory flow (PEF), functional residual capacity (FRC), and forced expiratory flow rate at 25% of vital capacity (FEF25%)], the mental health of family members, and their satisfaction with nursing care.
Results: The total effective treatment rate was 77.5% in the observation group and 97.5% in the experimental group, with the latter significantly higher (P<0.05). The duration of pulmonary rales and the length of hospitalization were significantly less in the experimental group (all, P<0.05). Post-intervention, the levels of PEF, FRC, and FEF25% showed substantial improvement in the experimental group compared to the observation group (all, P<0.05). Moreover, the Self-Rating Anxiety Scale (SAS) and Self-Rating Depression Scale (SDS) scores for family members in the experimental group were significantly lower than those in the observation group (all, P<0.05). Family satisfaction rates were 75.0% for the observation group and 97.5% for the experimental group, with the latter demonstrating significantly greater satisfaction with nursing care (P<0.05).
Conclusion: The hierarchical chain nursing model proves to be highly effective in managing pneumonia in children. This model not only enhances clinical outcomes and expedites the resolution of symptoms such as fever, cough, and pulmonary rales but also improves lung function and reduces psychological stress among family members. Consequently, this model significantly increases family satisfaction with nursing services.
Keywords: hierarchical chain care model, pneumonia, children, disappearance of fever, disappearance of cough, facilitation
1 INTRODUCTION
Pneumonia is a widespread clinical condition, predominantly affecting preschool-aged children[1]. The disease can present with various symptoms, including cough, dyspnea, and shortness of breath. In severe instances, it may lead to critical complications such as seizures, respiratory failure, heart failure, and can even pose a life-threatening risk to patients[2]. In recent years, the persistent rise in global environmental pollution has contributed to an increasing trend in pneumonia incidence[3]. Research indicates that young children, due to their immature immune systems and developmental factors, face a significantly higher risk of disease progression compared to adults[4]. Therefore, it is crucial to provide prompt and effective treatment for children diagnosed with pneumonia. Timely intervention is vital for facilitating symptom recovery and improving overall patient prognosis.
Traditionally, treatment strategies for pediatric pneumonia have included both symptomatic and causal interventions, employing antibiotics, antitussives, expectorants, and nebulization to manage disease progression[5]. While these methods have been effective, challenges persist, particularly in younger patients who may have limited understanding, immature cognitive development, and poor adherence to treatment protocols, which can hinder optimal outcomes[6]. Consequently, there is a pressing need for standardized, comprehensive, and systematic nursing interventions throughout the treatment process.
Recent studies suggest that the evolving demands for enhanced treatment outcomes and nursing quality in pediatrics have rendered traditional nursing models inadequate for the current healthcare landscape[7]. Some research advocates for the implementation of the hierarchical chain nursing model in pediatric care to improve nursing quality and support the rehabilitation of children[8]. This model emphasizes the stratification of nursing staff and delineates the responsibilities of different levels of nursing personnel, effectively addressing the diverse needs of pediatric patients. Furthermore, it reinforces accountability among nursing staff and enhances overall care efficiency and quality[9]. To assess the impact of the hierarchical chain nursing model on pediatric pneumonia management, this study analyzed 80 children diagnosed with pneumonia at our hospital between January 2020 and May 2022. The findings are presented in the following sections.
2 MATERIALS AND METHODS
2.1 Participants
This study included 80 children diagnosed with pneumonia who were admitted to our hospital between March 2021 and January 2022. We collected essential demographic data, including gender, age, duration of illness, type of infection, and educational levels of family members. The participants were divided into two groups-an observation group and an experimental group-each consisting of 40 cases, based on the nursing approaches employed. The study received approval from our hospital’s Ethics Committee, and informed consent was obtained from the families of all participants[10].
2.2 Inclusion and Exclusion Criteria
Inclusion Criteria:
(1) Children diagnosed with pneumonia based on relevant clinical test results.
(2) Availability of complete clinical data.
(3) Normal growth and development without significant pre-existing medical conditions.
(4) Guardians capable of cooperating with the study.
Exclusion Criteria:
(1) Children with other pulmonary diseases.
(2) Children with tuberculosis or congenital lung disorders.
(3) Children diagnosed with severe pneumonia.
(4) Children with significant organ dysfunction.
(5) Children with known allergies or contraindications to the medications or interventions used in this study.
(6) Children suffering from allergic rhinitis, pharyngitis, bronchitis, or other conditions that could confound study results.
(7) Children or their families with mental health issues or cognitive, communication, or other functional impairments.
(8) Children with incomplete clinical data.
(9) Patients unable to fully cooperate with the study for any reason.
2.3 Methods
2.3.1 Treatment Methods
Conventional treatments included the use of expectorants, cough suppressants, and bronchodilators. Oxygen therapy was administered as necessary to correct electrolyte and acid-base imbalances. Antibiotic therapy was initiated with broad-spectrum antibiotics until culture results were confirmed. For children with elevated fevers, prompt rehydration and cooling measures were implemented.
2.3.2 Nursing Care in the Observation Group
Children in the observation group received standard nursing interventions, which included administering medications as prescribed by the physician while closely monitoring changes in the child’s condition, including consciousness, mental state, and pupil response. Nurses prepared for potential emergencies and provided a comfortable ward environment, maintaining a temperature of approximately 18°C and humidity around 60%, along with regular ventilation and disinfection. They also addressed any inquiries from family members.
2.3.3 Nursing Care in the Experimental Group
Children in the experimental group received a hierarchical chain nursing intervention. Nursing staff were stratified into three levels (N1, N2, N3) based on their experience and qualifications. Nurses at the N1 level, who had 1-3 years of experience, focused on basic nursing tasks, including positioning care, dietary management, and vital signs monitoring. They ensured children were comfortably positioned, provided low-flow oxygen as needed, and instructed families on appropriate nutrition. N2-level nurses, with over three years of experience, executed more complex nursing procedures, such as airway management and emergency response, ensuring strict adherence to aseptic techniques and monitoring for fever. Meanwhile, N3-level nurses, who had at least ten years of experience, oversaw the overall nursing care, organized professional training, and conducted regular ward rounds to supervise N1 and N2 nurses. This collaborative approach ensured comprehensive and effective nursing care for children with pneumonia, with each level of nursing staff playing a crucial role in delivering targeted interventions and support.
2.4 Outcome Measures
(1) Clinical Treatment Outcome:
Cured: The child’s body temperature returned to normal, and symptoms such as cough and lung rales completely resolved.
Markedly Effective: The child’s body temperature normalized, and there was significant improvement in cough and lung rales.
Effective: The child’s body temperature and associated symptoms showed improvement, but did not meet the criteria for marked effectiveness.
Ineffective: There was no significant improvement in the child’s body temperature or symptoms, or they worsened.
(2) Symptom Resolution Time and Length of Hospitalization: The symptoms monitored in this study included fever, cough, and lung rales. The time taken for these symptoms to resolve and the total duration of hospitalization were recorded by medical staff.
(3) Pulmonary Function Indicators: The pulmonary function metrics assessed in this study included peak expiratory flow rate (PEF), functional residual capacity (FRC), and forced expiratory flow rate at 25% of vital capacity (FEF25%). These indicators were measured using an air blow test and lung function detector, with the average of three measurements taken for each child.
(4) Mental State of Family Members: The anxiety levels of family members were assessed before and after nursing interventions using the Self-Rating Anxiety Scale (SAS), where a lower score indicates reduced anxiety. Additionally, the Self-Rating Depression Scale (SDS) was employed to evaluate the depression levels of family members, with a total score of 100 points and a cutoff value of 53, where lower scores indicate less depression.
(5) Family Satisfaction with Nursing Care: Family satisfaction was assessed using the “Nursing Satisfaction Survey Scale” developed by our hospital. This scale consists of 20 questions, with each question rated on a 5-point scale. A total score of less than 70 indicates dissatisfaction, scores between 70 and 89 signify satisfaction, and scores of 90 or above denote very high satisfaction. Satisfaction is calculated as: Satisfaction=(Very Satisfied+Satisfied)/total cases×100%
2.5 Statistical Analysis
Data analysis was conducted using GraphPad Prism 8 and SPSS 25.0. For comparative analysis of measurement data, a t-test was employed, with results expressed as means (±s). Categorical data were analyzed using the chi-squared (x²) test, presented as n (%). A p-value of less than 0.05 was considered statistically significant.
3 RESULTS
3.1 Baseline Characteristics
In the observation group, there were 40 children, comprising 24 males and 16 females. Ages ranged from 18 months to 14 years, with a mean age of (4.77±3.10) years. The duration of illness varied from 0.4 to 3.3 years, with an average duration of (2.12±0.47) years. Infection types included 19 bacterial cases, 16 viral cases, and 5 mycoplasma cases. Regarding family educational levels, 12 children had parents with a high school education or below, while 28 had parents with a college education or higher. In the experimental group, also consisting of 40 children, there were 23 males and 17 females. Ages ranged from 20 months to 10 years, with an average age of (4.24±2.02) years. The duration of illness ranged from 0.5 to 3.6 years, with a mean of (2.17±0.52) years. Infection types included 17 bacterial cases, 16 viral cases, and 7 mycoplasma cases. In this group, 14 children had parents with a high school education or below, while 26 had parents with a college education or higher. The basic demographic data between the two groups were comparable, with no significant differences observed (P>0.05). (Table 1)
Table 1. Comparison of Basic Data
|
Observation Group (n=40) |
Experimental Group (n=40) |
t/χ² |
P |
Gender |
|
|
0.052 |
0.820 |
Male |
24 |
23 |
|
|
Female |
16 |
17 |
|
|
Age |
18months - 14 years old |
20 months - 10 years old |
|
|
Average age (years) |
4.77±3.10 |
4.24±2.02 |
0.803 |
0.427 |
Disease duration (years) |
0.4-3.3 |
0.5-3.6 |
|
|
Average duration of disease (years) |
2.12±0.47 |
2.17±0.52 |
-0.451 |
0.653 |
Infection type |
|
|
0.444 |
0.505 |
Bacterial |
19 |
17 |
|
|
Viral |
16 |
16 |
|
|
Mycoplasma |
5 |
7 |
|
|
Education level of family members |
|
|
0.228 |
0.633 |
High school and below |
12 |
14 |
|
|
College and above |
28 |
26 |
|
|
3.2 Comparison of Clinical Treatment Effects
The overall effective treatment rate in the observation group was 77.5%, compared to 97.5% in the experimental group. The treatment effectiveness in the experimental group was significantly greater than that in the observation group (P<0.05). (Table 2)
Table 2. Comparison of Clinical Treatment Effects
Group |
Number of Cases |
Cure |
Markedly Effective |
Efficient |
Invalid |
Total Effective Rate (%) |
Observation group |
40 |
7 |
11 |
13 |
9 |
31 (77.5%) |
Test Experimental group |
40 |
14 |
15 |
10 |
1 |
39 (97.5%) |
χ² |
- |
- |
- |
- |
|
7.314 |
P |
- |
- |
- |
- |
|
0.007 |
3.3 Comparison of Symptom Disappearance Time and Hospitalization Time
The time required for the resolution of symptoms (fever, cough, and pulmonary rales) and the length of hospitalization in the experimental group were significantly shorter than those in the observation group (all P<0.05). (Table 3)
Table 3. Comparison of Symptom Disappearance Time and Hospitalization Time (d)
Group |
Number of Cases |
Symptom Disappearance Time |
Hospital Stay |
||
Fever |
Cough |
Pulmonary Rales |
|||
Observation group |
40 |
4.82±0.35 |
8.54±0.67 |
7.78±0.69 |
9.83±2.01 |
Experimental group |
40 |
2.71±0.29 |
6.33±0.48 |
6.04±0.52 |
6.85±1.23 |
t |
- |
29.359 |
16.959 |
12.737 |
8.459 |
P |
- |
<0.001 |
<0.001 |
<0.001 |
<0.001 |
3.4 Comparison of the Levels of Related Indicators of Lung Function
As shown in Figure 1, the PEF values for the observation group before and after nursing interventions were (47.62±4.61, 59.28±6.45), while the FRC values were (68.92±6.47, 82.68±7.64) and the FEF25% values were (42.53±4.34, 49.98±5.23). In the experimental group, the PEF values before and after nursing were (47.56±4.63, 66.78±7.14), with FRC values of (68.85±6.52, 91.32±7.35) and FEF25% values of (42.58±4.41, 54.69±5.77). Comparisons of PEF, FRC, and FEF25% before nursing showed no significant differences between the two groups (all P>0.05). However, after nursing, the PEF, FRC, and FEF25% levels in the experimental group were significantly higher than those in the observation group (all P<0.05).
|
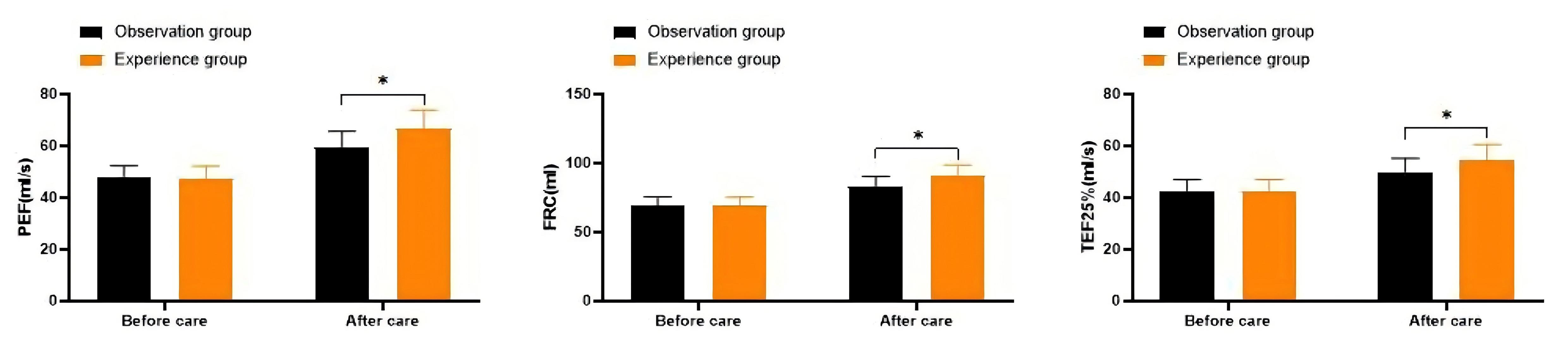
Figure 1. Comparison of the Levels of Related Indicators of Lung Function. Notes: *means P<0.05.
3.5 Comparison of Mental State Levels of Children’s Family Members
As illustrated in Figure 2, the SAS scores for the observation group before and after nursing care were (59.42±8.26, 54.37±7.32), while the SDS scores were (57.38±7.62, 50.07±5.84). In contrast, the SAS scores for the experimental group before and after nursing were (60.21±8.94, 47.73±6.85), and the SDS scores were (58.39±8.13, 42.62±5.39). Comparisons of SAS and SDS scores prior to nursing care indicated no significant differences between the two groups (all P>0.05). However, after nursing care, the SAS and SDS scores in the experimental group were significantly lower than those in the observation group (all P<0.05).
|
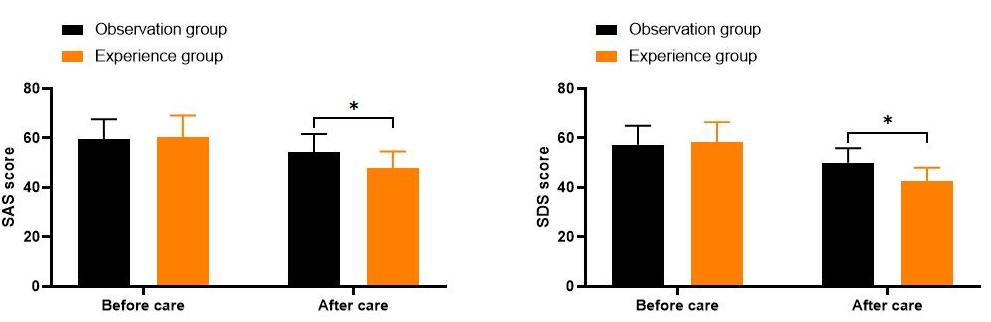
Figure 2. Comparison of Mental State Levels of Children’s Family Members. Notes: *means P<0.05.
3.6 Comparison of the Satisfaction of Children’s Family Members with Nursing Work
Family satisfaction rates were 75.0% in the observation group and 97.5% in the experimental group. (Table 4)
Table 4. Comparison of the Satisfaction of Children’s Family Members with Nursing Work
Group |
Number of Cases |
Very Satisfied |
Satisfy |
Dissatisfied |
Total Satisfaction (%) |
Observation group |
40 |
9 |
21 |
10 |
30 (75.0%) |
Test group |
40 |
16 |
23 |
1 |
39 (97.5%) |
χ² |
- |
- |
- |
- |
8.889 |
P |
- |
- |
- |
- |
0.003 |
4 DISCUSSION
Pneumonia is a prevalent condition among preschool children, with incidence peaks typically occurring in winter and spring. Due to factors such as immature respiratory development and lower overall resistance, young children are at a higher risk for pneumonia compared to adults[11]. Research indicates that pneumonia can progress rapidly, and timely treatment is crucial for positive outcomes. Therefore, effective treatment and nursing interventions are essential to safeguard children’s health.
In 2010, the Chinese Ministry of Health emphasized the importance of high-quality nursing services. With the continuous improvement of living standards, expectations for hospital nursing care have also risen. As a result, enhancing the quality of clinical nursing services has become a primary objective for healthcare institutions[12,13]. Studies have shown that conventional nursing practices often lead to inconsistent quality of care, largely due to variations in individual nurses’ skills and motivation. This inconsistency has resulted in unsatisfactory evaluations from patients and their families regarding clinical treatment and nursing services[14].
In response to the evolving needs of families, particularly in pediatric care, traditional nursing models are increasingly seen as inadequate. This study explored the implementation of a hierarchical chain nursing model in the management of children with pneumonia. This model categorizes nursing staff into three levels-N1, N2, and N3-based on their education and experience, with each level having distinct responsibilities. N1 nurses focus on basic care tasks such as monitoring vital signs and providing health education. N2 nurses carry out specific nursing procedures as directed by physicians, including airway management and emergency care. N3 nurses oversee overall care coordination, ensuring effective communication and management within the nursing team[15-17].
The findings of this study indicated that the total effective treatment rate was significantly higher in the experimental group (97.5%) compared to the observation group (77.5%) (P<0.05). Additionally, the time taken for symptoms such as fever, cough, and pulmonary rales to resolve, as well as the length of hospitalization, were significantly shorter in the experimental group. Furthermore, lung function indicators were significantly improved in the experimental group post-nursing.
These results are consistent with previous studies that have shown the hierarchical chain nursing model’s effectiveness in enhancing clinical outcomes for pediatric patients[18,19]. The model allows for clear delineation of responsibilities, minimizing confusion and ensuring comprehensive care. This structured approach can significantly reduce potential safety risks during nursing care, facilitating smoother treatment processes and accelerating recovery.
Moreover, the psychological well-being of family members is critical during a child’s illness. Previous research highlights that lack of knowledge about the illness can lead to increased anxiety and fear among family members, which may negatively impact treatment outcomes[20]. In this study, the anxiety and depression scores (SAS and SDS) for the experimental group were significantly lower post-intervention compared to the observation group. This improvement may be attributed to the hierarchical chain nursing model’s focus on addressing the psychological needs of families and regularly updating them on their child’s condition.
Family satisfaction with nursing care also significantly differed between groups, with 97.5% satisfaction in the experimental group compared to 75.0% in the observation group (P<0.05). This indicates strong approval and recognition of the hierarchical chain nursing model among families.
Limitations
Despite these promising results, this study has several limitations. First, the sample size was relatively small, which may affect the generalizability of the findings. Second, the study was conducted at a single institution, limiting the diversity of the patient population. Future research should involve larger, multi-center studies to validate these findings further. Additionally, while the hierarchical chain nursing model showed positive outcomes, further exploration into potential barriers to implementation and staff training needs is warranted. Finally, long-term follow-up studies are needed to assess the enduring effects of this nursing model on both clinical outcomes and family satisfaction.
5 CONCLUSION
In conclusion, the hierarchical chain nursing model demonstrates significant potential in improving treatment efficacy, promoting symptom resolution, enhancing pulmonary function, and alleviating psychological distress among families of children with pneumonia. This model not only improves clinical outcomes but also increases family satisfaction with nursing care, highlighting its relevance in contemporary pediatric healthcare.
Acknowledgements
Not applicable.
Conflicts of Interest
The authors declared no conflict of interest.
Ethical Statement
The study was approved by the Ethics Committee of Hengshui People’s Hospital (No. I1398.405).
Author Contribution
Lu J was responsible for the overall research design and methodology formulation. Chang T conducted data collection and analysis, and drafted the initial manuscript. Hao M performed an important literature review and provided valuable theoretical support. Liu L was in charge of creating figures and data visualization, ensuring the clear presentation of research findings. Yin Z edited the manuscript for language and formatting, enhancing the overall quality of the paper. All authors reviewed and revised the final version of the research, ensuring the accuracy and consistency of the study.
Abbreviation List
FEF25%, Forced expiratory flow rate at 25% of vital capacity
FRC, Functional residual capacity
PEF, Peak expiratory flow rate
SAS, Self-rating anxiety scale
SDS, Self-rating depression scale
References
[1] Yun KW, Wallihan R, Juergensen A et al. Community-acquired pneumonia in children: myths and facts. Am J Perinatol, 2019; 36: S54-S57.[DOI]
[2] Florin TA, Ambroggio L, Brokamp C et al. Biomarkers and Disease Severity in Children With Community-Acquired Pneumonia. Pediatrics, 2020; 145: e20193728.[DOI]
[3] Fritz CQ, Edwards KM, Self WH et al. Prevalence, Risk Factors, and Outcomes of Bacteremic Pneumonia in Children. Pediatrics, 2019; 144: e20183090.[DOI]
[4] Masarweh K, Gur M, Toukan Y et al. Factors associated with complicated pneumonia in children. Pediatr Pulm, 2021; 56: 2700-2706.[DOI]
[5] Nascimento-Carvalho CM. Community-acquired pneumonia among children: The latest evidence for an updated management. J Pediatr, 2020; 96: 29-38.[DOI]
[6] Zhang R, Wang H, Tian S et al. Adenovirus viremia may predict adenovirus pneumonia severity in immunocompetent children. BMC Infect Dis, 2021; 21: 213.[DOI]
[7] Sharma PK, Vinayak N, Aggarwal GK et al. Severe Necrotizing Pneumonia in Children: A Challenge to Intensive Care Specialist. J Trop Pediatr, 2020; 66: 637-644.[DOI]
[8] Pickler RH. Supply Chain for Nursing Science. Nurs Res, 2022; 71: 337-338.[DOI]
[9] Hu J, Zhou L, Ding J. Application of Chain Nursing Process in the Nursing of Elderly Inpatients with Implantable Venous Infusion Port. Emerg Med Int, 2022; 2022: 5496533.[DOI]
[10] Zhu Y, Xu B, Li C et al. A Multicenter Study of Viral Aetiology of Community-Acquired Pneumonia in Hospitalized Children in Chinese Mainland. Virol Sin, 2021; 36: 1543-1553.[DOI]
[11] Dean P, Schumacher D, Florin TA. Defining Pneumonia Severity in Children: A Delphi Study. Pediatr Emerg Care, 2021; 37: e1482-e1490.[DOI]
[12] Nandan D, Mittal H, Sharma A et al. Thinking beyond infections in children with recurrent/persistent pneumonia. Trop Doct, 2021; 51: 356-361.[DOI]
[13] Williams DJ, Creech CB, Walter EB et al. Short- vs Standard-Course Outpatient Antibiotic Therapy for Community-Acquired Pneumonia in Children: The SCOUT-CAP Randomized Clinical Trial. JAMA Pediatr, 2022; 176: 253-261.[DOI]
[14] Klompas M, Branson R, Cawcutt K et al. Strategies to prevent ventilator-associated pneumonia, ventilator-associated events, and nonventilator hospital-acquired pneumonia in acute-care hospitals: 2022 Update. Infect Cont Hosp Epidemiol, 2022; 43: 687-713.[DOI]
[15] Xiang S, Tang W, Shang X et al. Practice of Multidisciplinary Collaborative Chain Management Model in Constructing Nursing Path for Acute Trauma Treatment. Emerg Med Int, 2022; 2022: 1342773.[DOI]
[16] Zhang S, Akmar LZ, Bailey F et al. Cost of management of severe pneumonia in young children: systematic analysis. J Glob Health, 2016; 6: 010408.
[17] Miyagishima K, Matsui T, Obara T et al. Long-term care level as a predictor of a poor outcome in elderly patients with pneumonia. Nihon Ronen Igakkai zasshi. Jpn J Geriatr, 2015; 52: 260-268.[DOI]
[18] Pratt MTG, Abdalla T, Richmond PC et al. Prevalence of respiratory viruses in community-acquired pneumonia in children: A systematic review and meta-analysis. Lancet Child Adolesc, 2022; 6: 555-570.[DOI]
[19] Rueda ZV, Aguilar Y, Maya MA et al. Etiology and the challenge of diagnostic testing of community-acquired pneumonia in children and adolescents. BMC Pediatr, 2022; 22: 169.[DOI]
[20] de Benedictis FM, Carloni I. Management of necrotizing pneumonia in children: Time for a patient-oriented approach. Pediatr Pulmonol, 2019; 54: 1351-1353.[DOI]
Copyright © 2024 The Author(s). This open-access article is licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, sharing, adaptation, distribution, and reproduction in any medium, provided the original work is properly cited.


