Psychological Care Can Reduce Pain Intensity, Relieve Negative Emotions, and Improve the Quality of Life of Patients with Advanced Gastrointestinal Cancer
Jing Liang1, Xiaofeng Tian2, Wei Yang2*
1Department of Gastro-colorectal Surgery, China-Japan Union Hospital of Jilin University, Changchun, Jilin Province, China
2Department of Hepatobiliary and Pancreatic Surgery, China-Japan Union Hospital of Jilin University, Changchun, Jilin Province, China
*Correspondence to: Wei Yang, Department of Hepatobiliary and Pancreatic Surgery, China-Japan Union Hospital of Jilin University, 126 Sendai Dajie, Changchun, 130000, Jilin Province, China; Email: jlccyangwei@jlu.edu.cn
Abstract
Objective: This study aims to explore the application value of psychological care in patients with advanced gastrointestinal (GI) cancer.
Methods: We randomly assigned 210 patients with advanced GI cancer treated in our hospital to receive routine care interventions (101 patients, the regular group) or to receive psychological care interventions based on the routine care (109 patients, the research group). The outcomes of care interventions in the two groups were recorded.
Results: The scores of health education, ward management, care attitude, and care skills were all higher in the research group than those in the regular group (P<0.05). The two groups were not statistically different in the visual analog scale (VAS) score before intervention (P>0.05). After intervention, the VAS score markedly decreased in both groups, with lower VAS scores in the research group than in the regular group (P<0.05). In both groups, the scores of the Self-Rating Anxiety Scale (SAS) and the Self-Rating Depression Scale (SDS) after intervention were lower than those before intervention (P<0.05). After intervention, the SAS and SDS scores were markedly lower in the research group than in the regular group (P<0.05). After intervention, the Self-perceived Burden Scale (SPBS) score decreased in both groups, with markedly lower SPBS scores in the research group than in the regular group (P<0.05). The score of the EORTC Quality of Life Questionnaire Core 30 (QLQ-C30) increased in both groups after intervention, with higher QLQ-C30 scores in the research group than in the regular group (P<0.05). The care compliance rate and the care satisfaction level were higher in the research group than in the regular group (P<0.05).
Conclusion: Psychological care can remarkably relieve the negative emotions of patients with advanced GI cancer, enhance the care quality, improve the quality of life of patients, and reduce the self-perceived burden of patients.
Keywords: psychological care, advanced gastrointestinal cancer, pain, negative emotions, quality of life
1 INTRODUCTION
Gastrointestinal (GI) cancer, common in internal medicine department, mostly occurs in the esophagus, stomach, and large intestine, accounting for more than 50% of the total tumor morbidity and mortality[1]. The changing living environment and lifestyles of people, as well as the extension of human life, lead to a yearly increase in the incidence of GI cancer[2]. Due to the absence of early symptoms, patients cannot be diagnosed definitely in the early stage of GI cancer, and most patients are already in middle and advanced stages when diagnosed[3]. Patients with GI cancer are at a high risk of death. Surgery is a routine treatment for GI cancer, but patients with advanced GI cancer face greater difficulties in the surgical operations and a higher chance of postoperative recurrence[4,5]. Surgical pain and discomfort in patients, and the occurrence of malignant tumors can cause a series of negative emotions, such as anxiety, fear, depression, and even suicidal tendencies, which delays the recovery time or even aggravates the condition[6,7]. Therefore, high-quality care interventions are essential in the clinic.
In recent years, psychological care has received much attention. Developments in social psychology and medicine reveal the essential role of psychological factors in the occurrence and outcomes of tumors[8]. Psychological care, based on psychological theory, gives patients high-quality care with rich psychological knowledge and care experience to relax the body and mind, maximizing the efficacy of treatment, and effectively reducing the pain intensity[9,10]. Here we mainly explored the application value of psychological care interventions by observing the effect of psychological care on the pain intensity, negative emotions, and quality of life of patients with advanced GI cancer.
2 MATERIALS AND METHODS
2.1 Clinical Data of Patients
We enrolled 210 patients with advanced GI cancer treated in our hospital into this study. This study was approved by the ethics committee. All data and information were collected after obtaining the informed consent from patients. We assigned 101 patients receiving routine care intervention to the regular group, including 54 males and 47 females, with an average age of 56.13±8.54 years. We assigned 109 patients receiving psychological care intervention based on the routine care to the research group, including 60 males and 49 females, with an average age of 56.81±8.18 years.
Inclusion criteria: Patients undergoing examinations for routine functions at the time of admission; patients with relatively complete clinical data; patients accompanied by family members at the time of admission; patients without mental illness; patients capable of normal communication. Exclusion criteria: Patients with an expected survival of less than 3 months; patients with severe cardiopulmonary failure; patients who did not participate in the follow-up.
2.2 Comparison of Care Models in the Two Groups
Patients in the regular group received conventional perioperative care. Each patient had a personal case file. We regularly introduced disease-related knowledge and precautions to patients in order to improve their health knowledge. All patients were ordered to follow a strict diet tailored to their nutritional status, which requires smaller but more frequent meals and prohibits irritating foods, mainly with foods rich in protein and vitamins. We urged patients to exercise appropriately to maintain a positive attitude. We closely monitored the disease condition of patients and regularly reminded them of the medication time and dosage. The wards were regularly disinfected and kept comfortable and quiet with suitable humidity and temperature. We also supervised the patient's routine schedule to help them live a healthy lifestyle.
Patients in the research group received psychological care interventions based on the routine care. First, we conducted psychological assessments of patients at the time of admission from their personality characteristics, cultural level, and life skills. Then we analyzed the results of psychological assessments and provided care for patients with our psychological knowledge and care experience. In a gentle tone, we popularized the disease knowledge, explained the cause of the disease, and shared successful cases to enhance the confidence of patients. We introduced the surrounding environment and involving doctors to patients and called them friendly to build a good and harmonious relationship with patients. To divert the patient’s attention to the disease, we encouraged them to try muscle relaxation, breathing relaxation, music enjoyment, and even mild entertaining activities if their physical condition allows. We informed patients of the surgical outcomes after they recovered from the anesthesia to eliminate their worries. After surgery, we popularized the knowledge about the causes and mechanisms of pain and conducted certain counseling to relieve the patient's doubts and panic. Also, we informed patients of the matters needing attention after surgery and introduced self-care skills to the patient and their families to relieve their negative emotions via actively talking and understanding their true thoughts and main concerns. In addition to the psychological counseling, we suggested family members to pay more attention to the patient’s psychological changes and communicate with them to show warmth and care. For patients with severe psychological disorders, we turned to psychologists for professional psychological interventions.
2.3 Outcome Measures
The pain intensity of patients before and after intervention was assessed by the visual analog scale (VAS)[11]. The negative emotions of patients before and after intervention were assessed by the Self-rating Anxiety Scale (SAS) and the Self-Rating Depression Scale (SDS)[12]. The self-perceived burden of patients was assessed by the Self-perceived Burden Scale (SPBS)[13]. The quality of life of patients before and after intervention was evaluated by the EORTC Quality of Life Questionnaire Core 30 (QLQ-C30)[14]. The care compliance rate and satisfaction level of patients were recorded using related scales.
2.4 Statistical Analysis
In this study, data analysis and visualization were performed on GraphPad Prism 7 (GraphPad Software Inc., San Diego, CA, USA). The count data was represented by the number of cases/percentage [n(%)] and their inter-group comparison was analyzed by the chi-square test. The measurement data was represented by the mean±SD and their inter-group comparison was analyzed by the t-test. The comparison between before and post intervention was analyzed by the repeated measurement ANOVA. The LSD-t test was used for the post-hoc analysis. P<0.05 indicates a statistical difference.
3 RESULTS
3.1 Comparison of Clinical General Information of Patients
Details of clinical general information of patients are shown in Table 1. The two groups were not markedly different in sex, age, body mass index (BMI), place of residence, and disease type (P>0.05).
Table 1. Clinical General Information of Patients (mean±SD, n(%))
|
Research Group (n=109) |
Regular Group (n=101) |
χ2/t |
P |
Sex |
|
|
0.023 |
0.879 |
Male |
60(55.05) |
54(53.47) |
|
|
Female |
49(44.95) |
47(46.53) |
|
|
Age |
|
|
0.221 |
0.638 |
> 50 years |
73(66.97) |
70(69.31) |
|
|
≤ 50 years |
36(33.03) |
31(30.69) |
|
|
Average age (year) |
56.81±8.18 |
56.13±8.54 |
0.588 |
0.557 |
BMI (kg/m2) |
22.93±4.43 |
23.02±4.31 |
0.149 |
0.882 |
Place of residence |
|
|
0.296 |
0.586 |
Rural area |
41(37.61) |
35(34.65) |
|
|
Urban area |
68(62.39) |
66(65.35) |
|
|
Disease type |
|
|
2.386 |
0.665 |
Gastric cancer |
38(34.86) |
31(30.69) |
|
|
Esophageal cancer |
18(16.51) |
15(14.85) |
|
|
Rectal cancer |
16(14.68) |
23(22.77) |
|
|
Colon cancer |
24(22.02) |
21(20.79) |
|
|
Pancreatic cancer |
13(11.93) |
11(10.90) |
|
|
3.2 Comparison of Comprehensive Care Quality Between the Two Groups
Details of the comprehensive care quality of the two groups are shown in Table 2. The scores of health education, ward management, care attitude, and care skills were all higher in the research group than in the regular group (P<0.05).
Table 2. Comprehensive Care Quality in the Two Groups (mean±SD)
|
Health Education |
Ward Management |
Care Attitude |
Care Skills |
Research group (n=109) |
81.16±3.83 |
82.31±3.45 |
89.98±3.98 |
84.16±4.01 |
Regular group (n=101) |
77.31±4.13 |
79.81±3.09 |
79.18±3.76 |
82.91±3.93 |
t |
6.992 |
5.500 |
20.120 |
2.273 |
P |
<0.05 |
<0.05 |
<0.05 |
<0.05 |
3.3 Comparison of Pain Intensity of Patients between the Two Groups
The VAS scores of patients before and after intervention are shown in Figure 1. The two groups were not statistically different in the VAS score before intervention (P>0.05). After intervention, the VAS score markedly decreased in both groups, which was lower in the research group than in the regular group (P<0.05).
|
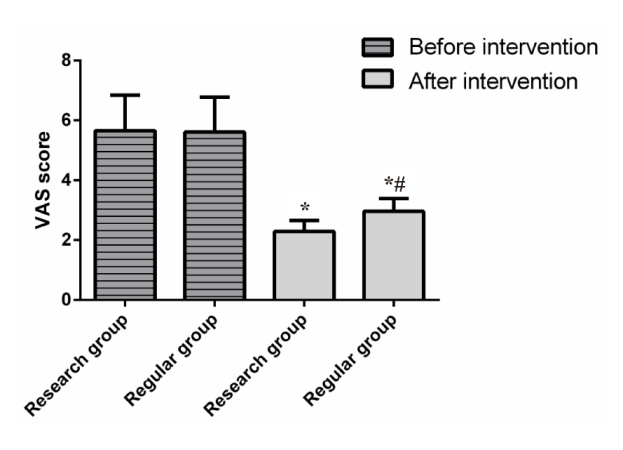
Figure 1. Pain Scores in the Two Groups. The two groups were compared in the VAS score before and after intervention. Notes: *P<0.05 when compared with data before intervention in the same group. #P<0.05 when compared with data in the research group after intervention.
3.4 Comparison of Scores of Negative Emotions Between the Two Groups
Scores of anxiety and depression of patients in the two groups are shown in Figure 2. The two groups were not statistically different in the SAS score and the SDS score before intervention (P>0.05). After intervention, the two scores decreased markedly in both groups, with markedly lower SAS and SDS scores in the research group than in the regular group (P<0.05).
|
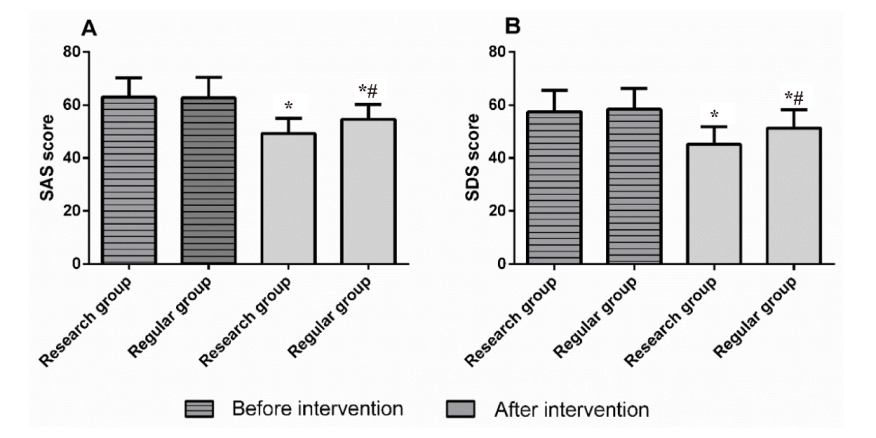
Figure 2. Scores of Negative Emotions in the Two Groups. A: Comparison of the SAS score between the research group and the regular group before and after intervention; B: Comparison of the SDS score between the research group and the regular group before and after intervention. Note: aP<0.05 when compared with data before intervention in the same group. bP<0.05 when compared with data in the research group after intervention.
3.5 Comparison of the Score of Self-Perceived Burden of Patients between the Two Groups
Details of the SPBS score of patients in the two groups are shown in Figure 3. The two groups were not statistically different in the SPBS score before intervention (P>0.05). After intervention, the SPBS score decreased markedly in both groups, which was lower in the research group than in the regular group (P<0.05).
|
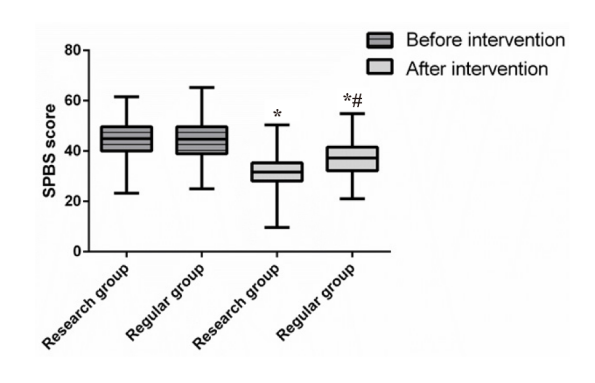
Figure 3. Scores of Self-perceived Burden of Patients in the Two Groups. The two groups were compared in the SPBS score before and after intervention. Notes: “*” indicates *P<0.05 when compared with data before intervention in the same group. “#” indicates #P<0.05 when compared with data in the research group after intervention.
3.6 Comparison of the Quality of Life of Patients in the Two Groups
The QLQ-C30 scores of patients before and after intervention in the two groups are shown in Figure 4. Before intervention, the two groups showed no differences in scores of role functioning (RF), emotional functioning (EF), cognitive functioning (CF), social functioning (SF), and physical functioning (PF) (P>0.05). After intervention, the scores of RF, EF, CF, SF, and PF increased in both groups, with higher scores in the research group than in the regular group (P<0.05).
|
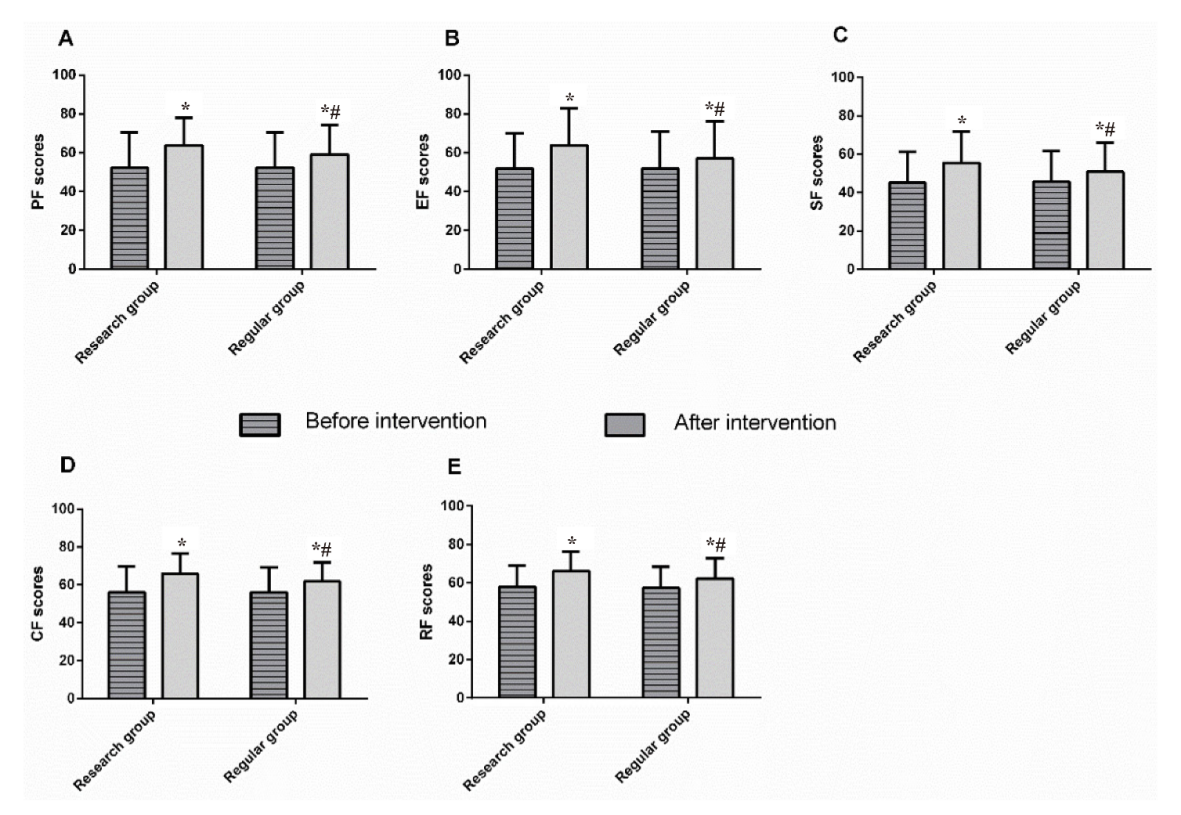
Figure 4. QLQ-C30 Scores in the Two Groups. A: Comparison of PF score between the research group and the regular group before and after intervention; B: Comparison of EF score between the research group and the regular group before and after intervention; C: Comparison of SF score between the research group and the regular group before and after intervention; D: Comparison of CF score between the research group and the regular group before and after intervention; E: Comparison of RF score between the research group and the regular group before and after intervention. Note: “*” indicates *P<0.05 when compared with data before intervention in the same group. “#” indicates #P<0.05 when compared with data in the research group after intervention.
3.7 Comparison of the Care Compliance Between the Two Groups
Details of the care compliance of patients in the two groups are shown in Table 3. The care compliance rate was markedly higher in the research group than in the regular group (93.58% vs. 84.16%, P<0.05).
Table 3. Survey of Care Compliance in the Two Groups [n (%)]
|
Complete Compliance |
Partial Compliance |
Noncompliance |
Compliance Rate |
Research group (n=109) |
48(44.04) |
54(49.54) |
7(6.42) |
93.58% |
Regular group (n=101) |
25(24.75) |
60(59.41) |
16(15.84) |
84.16% |
χ2 |
|
|
|
4.769 |
P |
|
|
|
0.029 |
3.8 Comparison of the Care Satisfaction Level Between the Two Groups
After care intervention, 0 cases of complaints were reported in the research group and 5 cases of complaints were reported in the regular group. The care satisfaction levels in the two groups are shown in Table 4. In the research group, 9 patients expressed dissatisfaction with the care work, with a satisfaction rate of 91.74%. In the regular group, 20 patients expressed dissatisfaction with the care work, with a satisfaction rate of 80.20%. The satisfaction rate was markedly higher in the research group than in the regular group (P<0.05).
Table 4. Survey of the Care Satisfaction in the Two Groups [n(%)]
|
Great Satisfaction |
Moderate Satisfaction |
Dissatisfaction |
Satisfaction Level |
Research group (n=109) |
61(55.96) |
39(35.78) |
9(8.26) |
91.74% |
Regular group (n=101) |
30(29.70) |
51(50.50) |
20(19.80) |
80.20% |
χ2 |
|
|
|
5.871 |
P |
|
|
|
0.015 |
4 DISCUSSION
The life-threatening GI cancer is induced by numerous factors, involving complex mechanisms[15]. Advanced GI cancer is a high-risk disease, so its management requires not only effective treatment but also intensive care interventions[16]. At present, care workers are indispensable in the medical team as an appropriate and effective care intervention is a major measurement of the medical quality[8,16]. Clinical care can minimize the damage caused by the disease, effectively reduce the pain intensity, and improve the quality of life of patients[17,18].
Psychological care interventions require care workers with certain communication skills and psychological counselling capacities, as well as a mastery of care skills and disease-related knowledge, who can promptly answer disease-related questions raised by patients and deal with emergencies calmly. Here we assessed the care quality of the two groups of care staff and found that the scores of health education, ward management, care attitude, and care skills were all higher in the research group than in the regular group. Such results indicate that psychological care interventions can improve the care quality and strengthen the sense of responsibility of medical staff to provide patients with more intimate, accurate, and timely services, which is beneficial to the following clinical treatment. When the tumor progresses to the advanced stage, the proliferation and metastasis of the tumor lesions will cause severe cancer pain in patients[19]. Therefore, it is critical to relieve the patient's cancer pain during the care interventions. The VAS is commonly used for the assessment of cancer pain[20]. In a previous study, rapid rehabilitation care remarkably reduced the VAS score of patients undergoing colorectal cancer surgery and relieved their pain intensity[21], suggesting that care intervention can moderately relieve postoperative pain. In this study, the VAS score was markedly lower in patients with advanced GI cancer receiving psychological care interventions than in patients receiving routine care. The lower VAS score in the research group may be a consequence of the good relationship between patients and care workers, and the positive measures such as psychological counseling, music therapy, and medication guidance, which effectively alleviate the pain of patients with GI cancer and give prompt solutions.
With rich experience of the care management of advanced tumors, now the care workers are mainly troubled by the difficulty to effectively relieve and alleviate the negative emotions[22,23]. Anxiety and depression are the most frequent negative emotions among patients with advanced cancer, which are generally assessed by the SAS and SDS[24]. A study proposed that high-quality care interventions can help reduce the burden of care and improve the mental health of patients with advanced cancer[25]. One another study also suggested that psychological care can help relieve the hospital anxiety and depression and enhance the quality of life of patients with colorectal cancer[26]. In the present study, the SAS and SDS scores in both groups after intervention were lower than those before intervention. After intervention, the SAS and SDS scores were markedly lower in the research group than in the regular group. Such results indicate that psychological care interventions are more effective in relieving negative emotions. During psychological care interventions, care workers mainly focus on the mental health issues of patients and communicate with patients based on their own personality characteristics to assess the psychological state of the patients, which notably relieve negative emotions of patients. Patients with advanced tumors are often subject to undesirable pressure due to factors such as family burden and economic burden, which is called self-perceived burden[27]. Self-perceived burden is a negative stress that impairs patients' physiological function, emotional function, and even quality of life[27,28]. Here, we assessed the self-perceived burden of patients and tested lower SPBS scores in the research group. Psychological care can correctly identify the psychological problems of patients and design personalized interventions to effectively handle them. Besides, care workers for psychological care make joint efforts with the patient's family members to show patients care and warmth to patients, so that they can keep a good psychological state with reduced self-perceived burden and cooperate with the treatment in an optimistic and positive attitude, which can improve the treatment effect and enhance the quality of life. GI cancer is a common malignant tumor that affects the quality of life of individuals[29]. A previous study revealed that self-care education can improve the QLQ-C30 score of patients with GI cancer receiving chemotherapy[29]. Here we assessed the quality of life of patients before and after intervention using the QLQ-C30 and noted an increase in the QLQ-C30 score in both groups after intervention, with a more sharp increase in the research group. Psychological care can not only relieve patients' pain intensity and negative emotions but also help patients develop good habits through interventions of life, diet, and medication. According to this study, care workers for psychological care encourage patients to maintain healthy interests and hobbies and create a comfortable and easing environment for patients to enhance their RF, EF, CF, SF, and PF. We also investigated the patient's compliance and satisfaction with care. Besides, the care compliance and the satisfaction level with the care were higher in patients receiving psychological care than in patients receiving routine care. Good patient-nurses relationships and joint efforts achieved by care workers and patients' family members facilitate the care work, improve the treatment experience, enhance the patient's compliance, and care satisfaction. Such findings provide a strong basis for the future promotion of clinical care work.
5 CONCLUSION
In summary, psychological care can remarkably relieve the negative emotions of patients with advanced GI cancer, enhance the care quality, improve the quality of life of patients, and reduce the self-perceived burden of patients. However, this study has some deficiencies. For example, we did not explore the application of psychological care in different GI cancer types, nor did we analyze the complications during the treatment and care interventions. We will overcome such deficiencies in future research.
Acknowledgements
Not applicable.
Ethical Statement
The study was approved by the Ethics Committee of the China-Japan Union Hospital of Jilin University.
Conflicts of Interest
The authors declared no conflict of interest.
Data Availability
No additional data beyond those presented in this paper are available.
Copyright Permissions
Copyright © 2021 The Author(s). Published by Innovation Forever Publishing Group Limited. This open-access article is licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, sharing, adaptation, distribution, and reproduction in any medium, provided the original work is properly cited.
Author Contribution
Yang W designed this study; Liang J and Yang W wrote the article; Liang J and Tian X collected the data and performed the statistical analysis; Tian X reviewed the manuscript; all authors approved the final version.
Abbreviation List
CF, Cognitive functioning
EF, Emotional functioning
GI, Gastrointestinal
PF, Physical functioning
QLQ-C30, Quality of Life Questionnaire Core 30
RF, Role functioning
SAS, Self-rating Anxiety Scale
SDS, Self-rating Depression Scale
SF, Social functioning
SPBS, Self-perceived Burden Scale
VAS, Visual analog scale
References
[1] Yuan W, Chen J, Shu Y et al. Correlation of DAPK1 methylation and the risk of gastrointestinal cancer: A systematic review and meta-analysis. PLoS One, 2017; 12: e0184959.[DOI]
[2] Yi L, Zhao T, Li YY et al. Analysis of incidence and mortality for upper digestive tract cancers and results of early detection and treatment program in Feicheng, Shandong Province. Zhonghua Yu Fang Yi Xue Za Zhi, 2017; 51: 403-408.[DOI]
[3] Du XM, Wang LH, Chen XW et al. Prognostic value of Sox2 expression in digestive tract cancers: A meta-analysis. J Huazhong Univ Sci Technolog Med Sci, 2016; 36: 305-312.[DOI]
[4] Urashima M, Ohdaira H, Akutsu T et al. Effect of vitamin D supplementation on relapse-free survival among patients with digestive tract cancers: The AMATERASU randomized clinical trial. JAMA, 2019; 321: 1361-1369.[DOI]
[5] Miyake KK, Nakamoto Y, Mikami Y et al. The predictive value of preoperative 18F-fluorodeoxyglucose PET for postoperative recurrence in patients with localized primary gastrointestinal stromal tumour. Eur Radiol, 2016; 26: 4664-4674.[DOI]
[6] Zvolensky M, Jardin C, Farris SG et al. Gut interpretations: how difficulties in emotion regulation may help explain the relation of visceral sensitivity with depression and anxiety among young adults with gastrointestinal symptoms. Psychol Health Med, 2018; 23: 840-845.[DOI]
[7] Zhang XK, Chen QH, Wang WX et al. Evaluation of dexmedetomidine in combination with sufentanil or butorphanol for postoperative analgesia in patients undergoing laparoscopic resection of gastrointestinal tumors: A quasi-experimental trial. Medicine, 2016; 95: e5604.[DOI]
[8] Wiener L, Battles H, Zadeh S et al. Gastrointestinal stromal tumor: psychosocial characteristics and considerations. Support Care Cancer, 2012; 20: 1343-1349.[DOI]
[9] Santangelo P, Procter N, Fassett D. Mental health nursing: Daring to be different, special and leading recovery-focused care? Int J Ment Health Nurs, 2018; 27: 258-266.[DOI]
[10] Loffler-Stastka H, Gelo O, Pleschberger I et al. Psychotherapy training in Austria: Baseline and socio-demographic background data from a SPRISTAD (Society of Psychotherapy Research Interest Section on Therapist Training and Development)-Pilotstudy. Z Psychosom Med Psychother, 2019; 65: 341-352.[DOI]
[11] Sung YT, Wu JS. The Visual Analogue Scale for Rating, Ranking and Paired-Comparison (VAS-RRP): A new technique for psychological measurement. Behav Res Methods, 2018; 50: 1694-1715.[DOI]
[12] Dunstan DA, Scott N, Todd AK. Screening for anxiety and depression: reassessing the utility of the Zung scales. BMC Psychiatry, 2017; 17: 329.[DOI]
[13] Ni Q, Cheng G, Chen A et al. Early detection of mental illness for women suffering high-risk pregnancies: an explorative study on self-perceived burden during pregnancy and early postpartum depressive symptoms among Chinese women hospitalized with threatened preterm labour. BMC Psychiatry, 2020; 20: 250.[DOI]
[14] Davudov MM, Harirchi I, Amiraliyev N et al. The Azeri Version of European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire (EORTC QLQ-C30): Translation and Validation. Asian Pac J Cancer Prev, 2020; 21: 267-271.[DOI]
[15] Ulrich CM, Himbert C, Holowatyj AN et al. Energy balance and gastrointestinal cancer: risk, interventions, outcomes and mechanisms. Nat Rev Gastroenterol Hepatol, 2018; 15: 683-698.[DOI]
[16] Westman B, Ullgren H, Olofsson A et al. Patient-reported perceptions of care after the introduction of a new advanced cancer nursing role in Sweden. Eur J Oncol Nurs, 2019; 41: 41-48.[DOI]
[17] Harmon J, Summons P, Higgins I. Experiences of the older hospitalised person on nursing pain care: An ethnographic insight. J Clin Nurs, 2019; 28: 4447-4459.[DOI]
[18] Igai Y. Effectiveness of non-pharmacological nursing interventions to improve the quality of life of patients with idiopathic pulmonary fibrosis: A systematic review. Jpn J Nurs Sci, 2019; 16: 241-252.[DOI]
[19] Xu L, Wan Y, Huang J et al. Clinical analysis of electroacupuncture and multiple acupoint stimulation in relieving cancer pain in patients with advanced hepatocellular carcinoma. J Cancer Res Ther, 2018; 14: 99-102.[DOI]
[20] Pardo J, Mena A, Jimenez E et al. Effectiveness of fentanyl pectin nasal citrate in controlling episodes of breakthrough cancer pain triggered by routine radiotherapy procedures. Clin Transl Oncol, 2019; 21: 1568-1572.[DOI]
[21] Xu F, Yu P, Li L. Rapid rehabilitation nursing in postoperative patients with colorectal cancer and quality of life. Oncol Lett, 2019; 18: 651-658.[DOI]
[22] Voogt E, Van Der Heide A, Van Leeuwen AF et al. Positive and negative affect after diagnosis of advanced cancer. Psychooncology, 2005; 14: 262-273.[DOI]
[23] Szczygiel DD, Mikolajczak M. Emotional intelligence buffers the effects of negative emotions on job burnout in nursing. Front Psychol, 2018; 9: 2649.[DOI]
[24] He Y, Sun LY, Peng KW et al. Sleep quality, anxiety and depression in advanced lung cancer: patients and caregivers. BMJ Support Palliat Care, 2020.[DOI]
[25] Trevino KM, Prigerson HG, Maciejewski PK. Advanced cancer caregiving as a risk for major depressive episodes and generalized anxiety disorder. Psychooncology, 2018; 27: 243-249.[DOI]
[26] Zhang X, Liu J, Zhu H et al. Effect of psychological intervention on quality of life and psychological outcomes of colorectal cancer patients. Psychiatry, 2020; 83: 58-69.[DOI]
[27] Oeki M, Takase M. Coping strategies for self-perceived burden among advanced cancer patients. Cancer Nurs, 2020; 43: E349-E355.[DOI]
[28] Fernandez De Larrinoa Palacios P, Martinez Rodriguez S, Ortiz Marques N et al. Family caregiver's self-perceived health status and its relation to burden. Psicothema, 2011; 23: 388-393.
[29] Xie J, Zhu T, Lu Q et al. The effects of add-on self-care education on quality of life and fatigue in gastrointestinal cancer patients undergoing chemotherapy. BMC Complement Med Ther, 2020; 20: 15.[DOI]


