Effects of Intervention of Fine Management Mode in Operating Room on Postoperative Infection Rate and Quality of Life of Patients Undergoing Gastrointestinal Surgery
Yan Hu1*
1Jianyang People's Hospital, Jianyang, Sichuan Province, China
*Correspondence to: Yan Hu, Jianyang People's Hospital, 180 Hospital Road, Jianyang 641400, Sichuan Province, China; Email: zhima1184744@163.com
Abstract
Objective: This study was designed to explore the influence of the intervention of fine management mode in the operating room on postoperative infection rate and quality of life of patients undergoing gastrointestinal surgery.
Methods: A total of 145 patients who underwent gastrointestinal surgery in our hospital from June 2019 to June 2020 were recruited and randomly divided into two groups, including 67 patients in the control group and 78 patients in the observation group. Patients in the former group received conventional management mode in the operating room, and patients in the latter group received fine management mode in the operating room. The postoperative infection rate and quality of life were compared between the two groups. The nursing quality and nursing satisfaction of patients were evaluated in both groups.
Results: Compared with the control group, patients in the observation group exhibited markedly lower postoperative infection rate and better postoperative wound healing condition. Besides, patients in the observation group had notably better quality of life, higher nursing quality, and higher nursing satisfaction than those in the control group, and the difference was statistically significant (P<0.05).
Conclusion: The intervention of fine management mode in the operating room can effectively reduce the postoperative infection rate and improve the quality of life of patients undergoing gastrointestinal surgery, leading to higher satisfaction.
Keywords: operating room, fine management mode, gastrointestinal surgery, postoperative infection rate, quality of life
1 INTRODUCTION
Since the gastrointestinal tract is a system that alternates between the human body and external objects, it is easy to have a variety of germs, causing gastrointestinal diseases, so gastrointestinal surgery is extremely common in surgery[1]. It has also been shown[2,3] that patients undergoing gastrointestinal surgery are highly susceptible to hospital-acquired infections after surgery, as most gastrointestinal surgical incisions are class II and III, and incision infections are typical complications and are highly prevalent in low- and middle-income countries. Patients experience postoperative pain, high body temperature, and infection due to the majority of bacteria that attack the patient's incision during the perioperative period, making the infection rate as high as 15% or more[4]. There are many factors give rise to infection, such as medical staff[5], air[6], environment in the operating room[7], surgical instruments[8] and patients themselves[9]. When surgical incision infection occurs, there is redness, swelling and fever in the incision, which will affect the wound healing. If it is not handled properly in time, it will deteriorate, causing serious damage to organ function and serious systemic infection. It can reduce the quality of life of patients, affect the prognosis, and even lead to death[10,11].
It is of great significance to take effective measures to reduce the incidence of postoperative incision infection, and fine management in the operating room is therefore important to prevent gastrointestinal incision infection[12]. This concept emphasizes on strengthening the management of operating room and strictly carrying out disinfection operation. It mainly includes visit before operating room nursing intervention (to give psychological intervention for patients, build their confidence in overcoming diseases, and avoid the decline of immunity caused by negative emotions), skin clean before operation (to reduce bacteria in skin and gastrointestinal tract), strict aseptic operation during operation, enhancement in disinfection of operating room articles, washes in time after operation, and the use of surgical dressing to cover the incisions (the surgical dressing should be change in time to promote wound healing)[13-15]. The nursing operation is refined from before surgery to after surgery, so that the operating room nursing becomes rigorous from simplicity, and the nursing risk decreases significantly. In this way, the scores of aseptic operation, nursing practice and health educationare all higher after surgery, and postoperative infection and other symptoms are less common in patients[16]. In this study, patients undergoing gastrointestinal surgery were treated with fine management intervention in the operating room to observe their postoperative infection rate and quality of life, as detailed below.
2 MATERIALS AND METHODS
2.1 Research Objects
A total of 145 patients undergoing gastrointestinal surgery in Jianyang People's Hospital were recruited from June 2019 to June 2020. They were randomly divided into an observation group and a control group. Seventy-eight patients in the observation group were treated with fine management mode in the operating room, and sixty-seven patients in the control group were treated with routine management mode. The observation group consisted of 45 males and 33 females, with a mean age of (36.2±1.5) years; The control group consisted of 35 males and 32 females, with a mean age of (35.9±1.3) years. Inclusion criteria: All the selected patients met the diagnostic criteria of functional gastrointestinal diseases, and had surgical indications; Patients had no other abnormal visceral function. After being examined by the Ethics Committee of our hospital, both patients and their families fully understood the research content and purpose, and voluntarily signed informed consent. Exclusion criteria: Patients were complicated with neurological or psychiatric diseases, serious chronic cardiovascular and cerebrovascular diseases, renal diseases, malignant tumors, or immunodeficiency diseases; Patients could not cooperate with the study. There was not considerable difference in general data between the two groups (P>0.05), which was comparable.
2.2 Methods
Control group: During the surgery, patients were given routine clinical nursing management, that is, their blood loss and blood oxygen saturation were observed routinely.
Observation group: During the surgery, the patients received fine management mode in operating room with excelsior and more thoughtful services. (1) Systematic targeted theoretical training and relevant practice were conducted for relevant personnel involved in the operation, so as to make all staff fully realize that the key of fine management is to refine service quality and work distribution. (2) Tools used in the operating room were required clearly. Medical supplies in the operating room had specific locating places, and the usage of each kind of supplies should be recorded accordingly. Different medical devices had corresponding management personnel to be responsible for, maintenance, management and repair. (3) All instruments in the operating room under the fine management mode were disinfected and sterilized on time, and relevant records were made. For some instruments that have been used for many times, bacteria detection should be carried out before use, so as to prevent unnecessary influence on the results of operation and reduce error rate. Moreover, all personnel entering the operating room must strictly abide by the principle of sterility. (4) Fine management of the operating room emphasized all-round management from the beginning to the end of the surgery. At the beginning, the doctors should have a comprehensive understanding of the patients, adjust the patients' mentality, and tell the patients the basic procedure of the operation. When the surgery was going on, the doctors concentrated on the operation and dealt with the accidents in time to ensure the smooth operation. At the end of the surgery, the doctors needed to analyze and deal with the patient's condition in time, actively communicate with the patient and ask about his condition and mood, guide the patient's diet and tell them to start with liquid food, so as to avoid the adverse situation caused by poor gastrointestinal peristalsis after the operation. Also, the doctors needed to pay attention to the patient's urine volume, frequency, color, shape, etc., medications, and report the adverse situation in time, thus accomplishing a finely managed operation.
2.3 Outcome Measures
In both groups, the wound infection of patients was counted, and the wound healing was evaluated: Healing grade A referred that the wound healed well and there was no adverse reaction; Healing grade B referred that the wound healed in general, with hematoma and effusion, butdid not fester; Healing grade C referred that there was suppuration at the incision of the patient that needed drainage.
The postoperative complications were compared between the two groups, including incision infection, incision dehiscence and abdominal abscess.
The nursing quality assessment form was used to score the sterility, completeness of nursing records, item management, nursing practice, basic knowledge assessment and health education of the two groups, with a full score of 100 for each item. The higher the score, the higher the nursing quality.
The nursing satisfaction of patients was counted in both groups: the questionnaire of nursing satisfaction was designed by our hospital, of which 90-100 was considered as great satisfied, 80-89 as satisfied, 70-79 as relatively satisfied, less than 70 as dissatisfied. The total satisfaction = great satisfied + satisfied.
The scores of postoperative quality of life between the two groups was compared: a Shot Form 36 Health Survey (SF-36) was applied to evaluate patients' quality of life, including physiological function, physical function, material life and social function, with a total score of 0-100. The higher the score, the better the quality of life.
2.4 Statistical Analysis
SPSS22.0 was applied to process the data. The measurement data was expressed as mean±SD. Paired t-test was utilized for intra-group comparison before and after treatment, and independent sample t-test for inter-group comparison. The enumeration data was expressed as cases (%), and χ2 test was applied for inter-group comparison. P<0.05 was considered statistically significant.
3 RESULTS
3.1 Wound Healing in the Two Groups
The infection rate of incision in the observation group was 1.3%, which was evidently lower than that in the control group (8.9%, P<0.05). The healing rate of grade A was 91.06% in the observation group, notably higher than that in the control group (77.6%, P<0.05); The healing rate of grade C was 2.6%, notably lower than that in the control group (8.9%, P<0.05); And no considerable difference could be found between the two groups in healing rate of grade B (P>0.05). More details are shown in Table 1.
Table 1. Wound Healing in the Two Groups
|
Healing Grade A |
Healing Grade B |
Healing Grade C |
Incision Infection Rate |
Control group (n=67) |
52 (77.6) |
8 (11.9) |
7 (10.5) |
6 (8.9) |
Observation group (n=78) |
71 (91.0) |
5 (6.4) |
2 (2.6) |
1 (1.3) |
χ2/t |
5.0391 |
1.3501 |
3.8481 |
4.6191 |
P |
0.0248 |
0.2452 |
0.0498 |
0.0316 |
3.2 Comparison of Nursing Quality between the Two Groups
The nursing quality of patients in the observation group was markedly higher than that in the control group in all aspects (sterility, completeness of nursing records, item management, nursing practice, basic knowledge assessment, and health education), and the difference was statistically significant (P<0.05), as shown in Table 2.
Table 2. Comparison of Sleep Quality between the Two Groups After Nursing
|
Sterility |
Completeness Of Nursing Records |
Item Management |
Nursing Practice |
Basic Knowledge Assessment |
Health Education |
Control group (n=67) |
91.45±1.21 |
97.44±1.87 |
94.35±2.03 |
91.29±2.56 |
90.34±3.34 |
95.52±1.24 |
Observation group (n=78) |
95.87±1.57 |
90.12±1.43 |
89.21±1.78 |
85.78±2.71 |
84.54±3.01 |
87.21±2.26 |
χ2/t |
18.7492 |
26.67 |
16.2454 |
12.5213 |
10.9961 |
26.8207 |
P |
<0.0001 |
<0.0001 |
<0.0001 |
<0.0001 |
<0.0001 |
<0.0001 |
3.3 Comparison of Postoperative Complications between the Two Groups
The incidence of postoperative complication was 5.0% in the observation group, which was lower than that in the control group (14.9%). The difference was statistically significant (P<0.05), as shown in Table 3.
Table 3. Comparison of Postoperative Complications between the Two Groups
|
Incision Infection |
Incision Dehiscence |
Abdominal Abscess |
Total |
Control group (n=67) |
6 (8.9) |
2 (3.0) |
2 (3.0) |
10 (14.9) |
Observation group (n=78) |
1 (1.3) |
1 (1.3) |
2 (2.4) |
4(5.0) |
χ2/t |
|
|
|
3.9661 |
P |
|
|
|
0.0464 |
3.4 Length of Stay, Hospitalization Expenses, and Nursing Satisfaction of Patients in Both Groups
Compared with the control group, the observation group exhibited shorter length of stay and lower hospitalization expenses (P<0.05). Moreover, the total satisfaction rate in the observation group was 91.0%, which was considerably higher than the control group (79.1%) (P<0.05). More details are shown in Table 4.
Table 4. Length of Stay, Hospitalization Expenses, and Nursing Satisfaction of the Two Groups of Patients
|
Length of Hospital Stay (d) |
Hospitalization Expenses (ten thousand yuan) |
Nursing satisfaction |
||||
Great Satisfied |
Satisfied |
Relatively Satisfied |
Dissatisfied |
Total Satisfaction |
|||
Control group (n=67) |
14.7±2.1 |
1.18±0.27 |
35 (52.2) |
18 (26.9) |
9 (13.4) |
6 (9.0) |
53 (79.1) |
Observation group (n=78) |
10.5±2.3 |
1.56±0.21 |
56 (71.8) |
15 (19.2) |
5 (6.4) |
2 (2.6) |
71 (91.0) |
χ2/t |
11.4096 |
9.52264 |
|
|
|
|
4.1361 |
P |
<0.0001 |
<0.0001 |
|
|
|
|
0.0420 |
3.5 Comparison of Quality of Life Scores between the Two Groups
Before management, no significant difference in the scores of quality of life could be found between the two groups (P<0.05). After management, the scores of physiological function, physical function, material life and social function in the observation group were notably higher than those in the control group, and the differences were statistically significant (P<0.05), as shown in Figure 1.
|
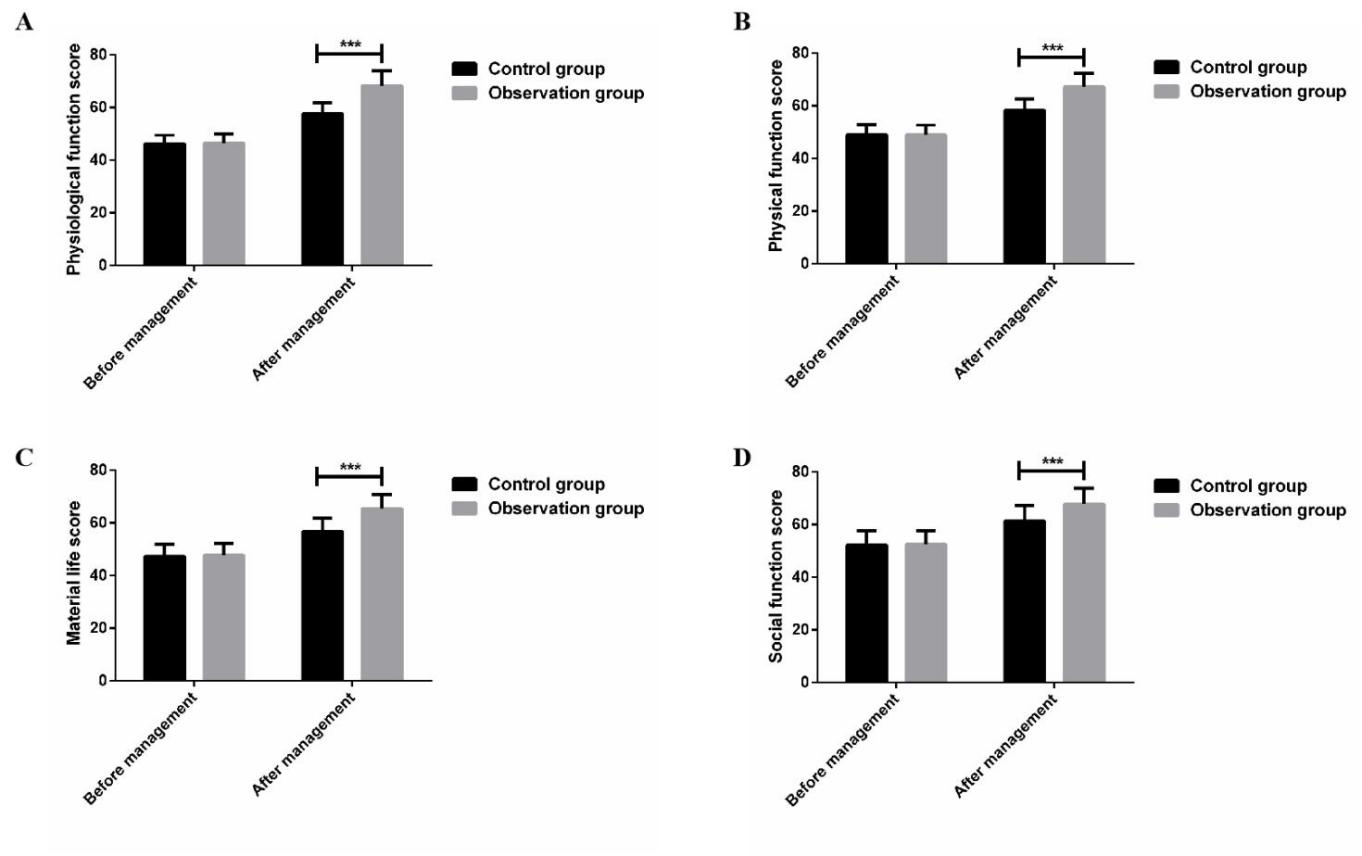
Figure 1. Comparison of Quality of Life Score Between the Two Groups. A: Comparison of physiological function score; B: Comparison of physical function score; C: Comparison of material life score; D: Comparison of social function score. *** P<0.001.
4 DISCUSSION
Operating room is an important technical department of the hospital, the largest open centralized treatment place, and one of the key departments of the hospital[17]. Operating room, as a working environment reflecting the high level of therapeutic medicine in the surgical field, needs to meet all functions required by surgery[18]. The air quality, strict disinfection and sterilization of surgical articles, and efficient and safe air purification system in operating room are vital factors to prevent surgical incision infection[19]. Besides, to create a safe, comfortable and clean operating environment for surgical patients is the purpose of the hospital, which should be considered by operating room managers. Operating rooms can be divided into aseptic purification operating rooms (Class I operating rooms), aseptic operating rooms (Class II operating rooms), bacterial operating rooms (Class III operating rooms), infection operating rooms (Class IV operating rooms) and special infection operating rooms (Class V operating rooms)[20,21]. Different operating rooms require different instruments and equipment, so it is advisable to have relatively fixed operating rooms for specialized surgeries, so as to create the most comfortable environment for medical staff. Fine management is first and foremost a scientific management method. To realize fine management, scientific and quantitative standards, operable and easy-to-execute operating procedures, and management work based on operating procedures must be established. It is a management method with the main goal of minimizing the resources occupied by management and reducing management costs[22].
In this paper, we studied the influence of intervention of fine management mode in the operating room on postoperative infection rate and quality of life of patients undergoing gastrointestinal surgery. The results showed that the postoperative infection rate of patients in the observation group who received fine management in the operating room was remarkably lower than that in the control group, along with better postoperative wound healing, shorter hospitalization time, and lower hospitalization expenses. There are many reports on the incidence of incision infections in gastrointestinal surgery in China[23,24], and one study[25] suggested that the incidence of incisioninfections after gastrointestinal surgery was 5.2%, and the occurrence of infections significantly increased medical costs, which is also validated in this research. The postoperative quality of life, nursing quality and nursing satisfaction of patients treated with fine management mode in the operating room were notably better than those who received conventional management, with statistically significant difference (P<0.05). The results have revealed that fine management mode in the operating room is comprehensive and systematic, and its application is mainly significant in terms of reducing the complication rate, shortening the length of stay of patients, and improving the quality of care. It not only standardizes and streamlines the treatment and nursing work, but also reduces the oversights due to the difference of individual abilities, effectively eliminates the bacterial source, cuts off the bacterial incision, and improves the nursing quality. Moreover, it improves the patient's quality of life and nursing satisfaction. The fine management mode in the operating room should be rigorous, meticulous, with standard sterilization operation, aseptic operation, operation evaluation, skin preparation, disease control, etc., to prevent blind spots. Treatments of pollutants, aseptic operation and surgical hygiene are carried out in strict accordance with rules and regulations to avoid the risk of infection. Health education and psychological care are also conducted for patients to build their confidence in overcoming diseases, as well as enhancement in disinfection management, incision wash and dressings placing. The invasion path of bacteria is blocked to eliminate the source of bacteria, so that the incidence of infection can be controlled.
5 Conclusion
To sum up, the utilization fine management mode in the operating room is conducive to reducing the postoperative infection rate of patients undergoing gastrointestinal surgery, improving the postoperative quality of life of patients, and strengthening the safety of nursing in the operating room, which is worthy of clinical promotion.
Acknowledgements
Not applicable.
Ethical Statement
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Jianyang People's Hospital.
Conflicts of Interest
The author declared no conflict of interest.
Data Availability
All data generated or analyzed during this study are included in this published article.
Copyright Permissions
Copyright © 2021 The Author(s). Published by Innovation Forever Publishing Group Limited. This open-access article is licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, sharing, adaptation, distribution, and reproduction in any medium, provided the original work is properly cited.
Author Contribution
Yan H collaboratively designed the study, collected data, analyzed data, and took part in writing the manuscript; all authors approved the final version.
References
[1] Guyton K, Alverdy JC. The gut microbiota and gastrointestinal surgery. Nat Rev Gastroenterol Hepatol, 2017; 14: 43-54.[DOI]
[2] Bhangu A, Ademuyiwa AO, Aguilera ML et al. Surgical site infection after gastrointestinal surgery in high-income, middle-income, and low-income countries: a prospective, international, multicentre cohort study. Lancet Infect Dis, 2018; 18: 516-525.[DOI]
[3] Thomas H. Describing the global burden of infection after gastrointestinal surgery. Nat Rev Gastroenterol Hepatol, 2018; 15: 190.[DOI]
[4] Wang Z, Chen J, Ren J et al. Surgical site infection following abdominal surgery in China: a multicenter cross-sectional study. Zhonghua Wei Chang Wai Ke Za Zhi, 2018; 21: 1366-1373.
[5] Takahashi Y, Takesue Y, Fujiwara M et al. Risk factors for surgical site infection after major hepatobiliary and pancreatic surgery. J Infect Chemother, 2018; 24: 739-743.[DOI]
[6] Brandt C, Hott U, Sohr D et al. Operating room ventilation with laminar airflow shows no protective effect on the surgical site infection rate in orthopedic and abdominal surgery. Ann Surg, 2008; 248: 695-700.[DOI]
[7] Salassa TE, Swiontkowski MF. Surgical attire and the operating room: role in infection prevention. J Bone Joint Surg Am, 2014; 96: 1485-1492.[DOI]
[8] Hashimoto D, Chikamoto A, Arima K et al. Unused sterile instruments for closure prevent wound surgical site infection after pancreatic surgery. J Surg Res, 2016; 205: 38-42.[DOI]
[9] Woodfield J, Deo P, Davidson A et al. Patient reporting of complications after surgery: what impact does documenting postoperative problems from the perspective of the patient using telephone interview and postal questionnaires have on the identification of complications after surgery? BMJ Open, 2019; 9: e028561.[DOI]
[10] Allegranzi B, Bischoff P, de Jonge S et al. New WHO recommendations on preoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis, 2016; 16: e276-e287.[DOI]
[11] Andrade LS, Siliprandi EMO, Karsburg LL et al. Surgical Site infection prevention bundle in cardiac surgery. Arq Bras Cardiol, 2019; 112: 769-774.[DOI]
[12] Loftus RW. Infection control in the operating room: is it more than a clean dish? Curr Opin Anaesthesiol, 2016; 29: 192-197.[DOI]
[13] Moszkowicz D, Hobeika C, Collard M et al. Operating room hygiene: Clinical practice recommendations. J Visc Surg, 2019; 156: 413-422.[DOI]
[14] Sánchez-Margallo FM, Sánchez-Margallo JA, Moyano-Cuevas JL et al. Use of natural user interfaces for image navigation during laparoscopic surgery: initial experience. Minim Invasive Ther Allied Technol, 2017; 26: 253-261.[DOI]
[15] Chinese Society of Surgical Infection and Intensive Care, Chinese Society of Surgery, Chinese Medical Association, Chinese College of Gastrointestinal Fistula Surgeons, Chinese College of Surgeons, Chinese Medical Doctor Association. Chinese guideline for the prevention of surgical site infection. Zhonghua Wei Chang Wai Ke Za Zhi, 2019; 22: 301-314.
[16] Grant MC, Hanna A, Benson A et al. Dedicated operating room teams and clinical outcomes in an enhanced recovery after surgery pathway for colorectal surgery. J Am Coll Surg, 2018; 226: 267-276.[DOI]
[17] Grant MC, Hanna A, Benson A et al. Improving operating room efficiency. Curr Urol Rep, 2019; 20: 28.[DOI]
[18] Dyas AR, Lovell KM, Balentine CJ et al. Reducing cost and improving operating room efficiency: examination of surgical instrument processing. J Surg Res, 2018; 229: 15-19.[DOI]
[19] Cosgrove MS. Infection control in the operating room. Crit Care Nurs Clin North Am, 2015; 27: 79-87.[DOI]
[20] Gaines S, Luo JN, Gilbert J et al. Optimum operating room environment for the prevention of surgical site infections. Surg Infect (Larchmt), 2017; 18: 503-507.[DOI]
[21] Katz JD. Control of the environment in the operating room. Anesth Analg, 2017; 125: 1214-1218.[DOI]
[22] Tsai MH, Sanford JA, Black IH et al. Operating room management at the edge of order and chaos. J Med Pract Manage, 2017; 32: 250-255.
[23] Xiao Y, Shi G, Zhang J et al. Surgical site infection after laparoscopic and open appendectomy: a multicenter large consecutive cohort study. Surg Endosc, 2015; 29: 1384-1393.[DOI]
[24] Cheng K, Li J, Kong Q et al. Risk factors for surgical site infection in a teaching hospital: a prospective study of 1,138 patients. Patient Prefer Adher, 2015; 9: 1171-1177.[DOI]
[25] Wang Z, Chen J, Wang P et al. Surgical site infection after gastrointestinal surgery in china: A multicenter prospective study. J Surg Res, 2019; 240: 206-218.[DOI]


