Taxane-based chemotherapy-induced peripheral neuropathy: a prospective cohort study
Ciara Power1, Xinqi Liu2*, Jamie Young1,2, Diana Munteanu1
1Department of Anaesthesia and Pain, Peter MacCallum Cancer Centre, Melbourne, Australia
2Department of Critical Care, The University of Melbourne, Melbourne, Australia
*Correspondence to: Xinqi Liu, Research Assistant, Department of Critical Care, The University of Melbourne, Grattan Street, Melbourne, 3010, Australia; Email: sheilaliu123@gmail.com
Abstract
Objective: Chemotherapy-induced peripheral neuropathy is a debilitating neurotoxic side effect of chemotherapy. Painful symptoms of CIPN can be chronic for cancer patients or survivors and limit their quality of life. Currently, chemotherapy-induced peripheral neuropathy is not well understood, there are no validated treatments available for patients, and the prevalence of the condition is not well-established in Australia. This study aimed to assess the incidence of chemotherapy-induced peripheral neuropathy within an Australian cohort of patients who had previously undertaken taxane-based chemotherapy agents paclitaxel or docetaxel. As a secondary outcome, this study aimed to identify any associated risk factors of CIPN and assess its impact on the QoL of patients.
Methods: This prospective cohort study assessed for CIPN through clinical diagnosis and used the Self-reported Leeds Assessment of Neuropathic Symptoms and Signs assessment tool for further support. Data was also collected on participants’ risk factor characteristics and symptom burden. Risk factors were analysed for correlation with CIPN using binary logistic regression tests.
Results: This study found an incidence rate of 36.9% for CIPN amongst 65 Australian participants who had undergone taxane-based chemotherapy. Symptoms persisted as chronic pain (>3 months) for 87.5% of participants with CIPN and smoking was found to be a significant risk factor associated with CIPN (OR=3.51, p<0.05).
Conclusion: This study established that a large proportion of chemotherapy patients experienced CIPN and its chronic pain symptoms, which impacted their QoL. Understanding CIPN prevalence and risk factors will improve future preventative measures and patient outcomes.
Keywords: chronic pain, taxane, chemotherapy-induced peripheral neuropathy
1 INTRODUCTION
Chemotherapy-induced peripheral neuropathy (CIPN) is a common and debilitating side effect seen in patients undergoing cancer treatments[1]. The condition is thought to be caused by damage to the peripheral nerves and is a result of neurotoxicity introduced into the body by chemotherapeutic drugs. There are four common clinical features of chemotherapy-induced peripheral neuropathy: pain and/or sensory changes in the hands and feet (paraesthesia, dysesthesia, heat/cold induced hyperalgesia, and mechanical allodynia), motor dysfunction (cramping, muscle weakness and effects on gait), symmetrical development of symptoms along limbs, and development of symptoms in a “glove-and-stocking” distribution, with the distal regions of the limbs experiencing the greatest deficits[1-3].
Varying drug types can also induce different clinical presentations in patients. Taxanes represent one of the classes of chemotherapeutic agents, with two of the most commonly used types being paclitaxel and docetaxel. These have proven to be effective in the treatment of highly prevalent malignancies, including but not limited to breast, lung, prostate, stomach, oesophageal, bladder, pancreas and ovarian[4]. However, taxanes were found to have one of the highest incidence rates of CIPN amongst all chemotherapeutic agents. Reported incidences of taxane-induced peripheral neuropathy vary from 13% to 62%[5], higher than that of cisplatin and vincristine[5]. Chemotherapy-induced peripheral neuropathy operates via numerous pathological pathways, but the exact underlying molecular mechanisms of action remain unknown. It is suggested that the pathology of taxane-induced peripheral neuropathy (TIPN) involves both direct damage to sensory neuron viability, and indirect, secondary effects of neuroinflammation. In particular, taxane-based CIPN is believed to occur under immune system-mediated processes, microglia-mediated processes and peripheral neuron dysfunctions[6].
CIPN can result in dosage limitations or even early cessation of cancer treatments, which can limit the chances of survival for cancer patients and increase cancer-related morbidity and mortality[7]. The burden of CIPN is not limited to simply the experience of pain but is extended to the global quality of life (QoL) of the patient and additional financial costs to the individual as well as the healthcare system[7,8]. In particular, the severity and number of CIPN symptoms were able to predict a reduced ability to work[9], showcasing a correlation between the severity of symptoms and reduced QoL.
In order to control and reduce the number of patients suffering from taxane-based CIPN, it is important to understand the clinical risk factors. Some of the postulated key risk factors that have been observed include increasing age, pre-existing baseline neuropathy, a higher number of chemotherapy cycles, alcohol consumption, diabetes, and smoking history[7,10]. Despite increasing interest in CIPN in recent years, many of its parameters remain uncertain. Consequently, studies on the prevalence and risk factors of CIPN have yet to establish a representative result. Literature specifically targeting the prevalence and risk factors of taxane-based CIPN in Australia is limited, and this raises concerns because many individuals in the Australian population continue to undergo these neurotoxic chemotherapy treatments.
The aim of this study is to identify the prevalence of taxane-based CIPN within an Australian cohort. As a secondary outcome, this study aims to analyse potential risk factors associated with CIPN within an Australian cohort using a validated assessment tool for neuropathic pain. Considerations were also given to assessing the impact of CIPN on patients’ QoL.
2 METHODS
2.1 Study Design
This was a prospective cohort study on patients who had previously undergone treatment with taxane-based chemotherapy between Jan 2017 to Jan 2018. Participants over the age of 18 were sourced via the Peter MacCallum Chemotherapy pharmacy records database and asked to complete surveys over the telephone. These data points were located in the pharmacy’s chemotherapy database and prescribing system. Eligible participants were contacted via telephone and verbal consent for the survey was obtained and documented.
2.2 Research Quality & Ethics Statement
This study was approved by the Peter MacCallum Cancer Centre Low and Negligible Risk Research Ethical Review Committee (HREC LNR/50136/PMCC-2019).
2.3 Participants
The inclusion criteria were patients over the age of 18, who were previously treated with the taxane-based chemotherapy agents paclitaxel or docetaxel.
The exclusion criteria included any participants with advanced progressive disease, at the end of life or deceased since treatment. Participants were also excluded if they were deemed inappropriate for a questionnaire for reasons such as personal circumstances or having a language barrier with no available interpreter. Participants that were known to have pre-existing diagnoses of peripheral nerve damage not related to chemotherapy, including symptoms of pain, sensory loss or decreased motor function, were also excluded.
2.4 Outcome Measures
The primary outcome measure of this study is the prevalence of chemotherapy-induced peripheral neuropathy in patients who undertook taxane-based chemotherapy. This was primarily assessed through clinical diagnosis by clinicians and further supported by the Self-reported Leeds Assessment of Neuropathic Symptoms and Signs (S-LANSS) questionnaire[11].Clinical diagnosis of CIPN was made by identifying the common signs and symptoms of CIPN such as pain in hands and feet, sensation of pins and needles and change in the colour of skin. Participants who were identified with CIPN through clinical diagnosis were then asked to complete the S-LANSS questionnaire to further support the neuropathic qualities of their pain. The S-LANSS is a tool tested and validated by the IASP Neuropathic Pain Special Interest Group and includes a series of questions related to the signs and symptoms of CIPN. Scoring a score of 12 or more on the S-LANSS questionnaire suggested that an individual’s pain was predominantly of neuropathic origin. In this study, the S-LANSS is only used as a secondary tool and participants who scored lower than 12 on the S-LANSS questionnaire were still capable of being diagnosed with CIPN through clinical diagnosis.
The impact of CIPN on the quality of life (QoL) of participants post-chemotherapy was a secondary outcome of this study. If CIPN pain was present, the pain was then graded as mild, moderate, severe, or life-threatening, based on the severity of impact on participants’ activities of daily living (ADLs), according to patients’ subjective report to questions in the survey. Grading of pain was made in conjunction with the Common Terminology Criteria for Adverse Events (CTCAE) 5.0 criteria. The CTCAE (version 5.0) is the most recent standardised definition for adverse events published by the National Cancer Institute (NCI) of the National Institutes of Health (NIH). This study used the CTCAE’s (version 5.0) definition of “neuralgia – a disorder characterised by intense painful sensation along a nerve or a group of nerves” as the criteria for neuropathic pain associated with chemotherapy toxicity.
Another secondary outcome measure of this study is the correlation between risk factors and CIPN occurrence. Potential risk factors investigated are increasing age, gender, smoking history, and adjuvant radiotherapy.
2.5 Statistical Analysis
Data on patient baseline characteristics were analysed using the IBM Statistical Package for Social Sciences (SPSS v29, 2022). Results for each characteristic were then presented descriptively and frequencies for each descriptive category were also represented as a percentage of the sample.
Correlations between risk factors and CIPN occurrence were analysed using Binary Logistic Regression Tests and presented as Odds Ratios (ORs) with 95% Confidence Intervals. Statistical significance was defined as a p-value less than 0.05 (p<0.05).
3 RESULTS
There were initially 109 eligible participants in this study, however, 18 were uncontactable and 23 did not consent or were since deceased. Of the final 68 participants included in this study, 3 had pre-existing neuropathic pain prior to chemotherapy and thus, only 65 participants who did not have pre-existing neuropathic pain were included in the primary analysis (Figure 1).
|
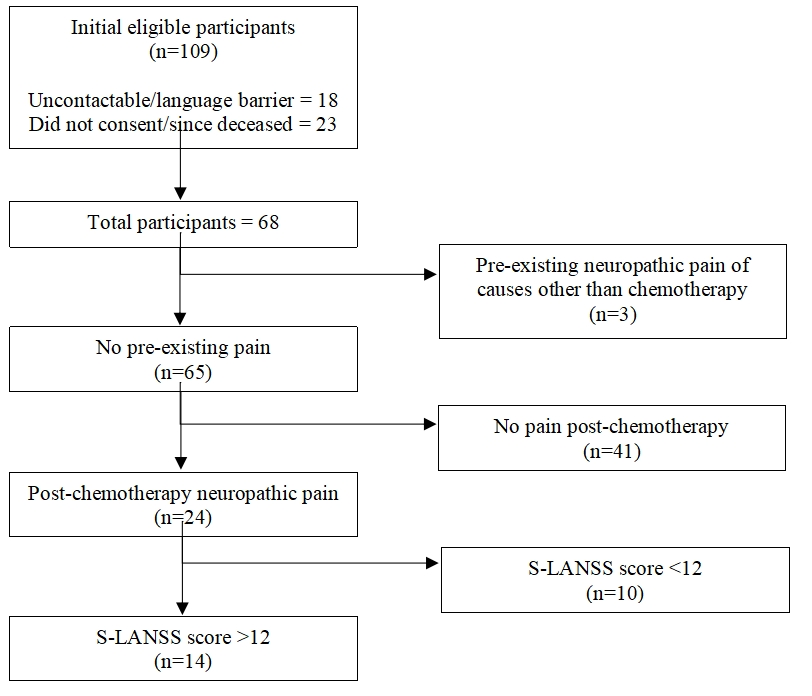
Figure 1. Participant Flow.
The mean age reported for the 68 participants in this study was 52 years (range 29-88) with a large proportion (82.4%) being female participants (Table 1). The majority (70.6%) of the participants had no smoking history but many had a higher-than-normal BMI score (High BMI: 38.2%, Obese BMI: 33.8%). Most participants in the study were patients with breast tumours, 53(77.9%), and the second largest group were patients belonging to the prostate tumour stream, 7(10.3%). Of the two types of taxanes used, 40 participants (58.8%) had used docetaxel whilst the remaining had paclitaxel. Participants (80.9%) commonly only had 1-10 cycles of chemotherapy, with only a small number of 3(4.4%) having more than 30 cycles. The combined treatment with radiotherapy was also quite common in this pool of participants, 44(64.7%).
Table 1. Participant Baseline Characteristics
Characteristics |
Frequency (n=68) |
Age (mean) |
52(Std. Deviation = 12.8) |
Sex (Female) |
56(82.4%) |
Smoking History |
|
Yes |
20(29.4%) |
No |
48(70.6%) |
BMI |
|
18.5-24.9 |
19(27.9%) |
25-29.9 |
26(38.2%) |
30-39.9 |
23(33.8%) |
Tumour Stream |
|
Breast |
53(77.9%) |
Gynaecology |
2(2.9%) |
Sarcoma |
2(2.9%) |
Prostate |
7(10.3%) |
Upper GI |
4(5.9%) |
Radiotherapy |
|
Yes |
44(64.7%) |
None |
24(35.3%) |
Taxane Type |
|
Paclitaxel |
28(41.2%) |
Docetaxel |
40(58.8%) |
Number of chemotherapy cycles |
|
1-10 |
55(80.9%) |
11-30 |
10(14.7%) |
31->50 |
3(4.4%) |
There were 65 participants included in the primary analysis and 24 (36.9%) participants who reported experiencing pain post chemotherapy were deemed as participants with CIPN (Table 2). Of those, 14 (58.3%) participants scored more than 12 on the S-LANSS assessment tool. Of the 24 participants who reported post-chemotherapy pain, 41.7% reported their pain levels as severe in their worst instances (Table 3), and 12.5% experienced severe impacts on their ADLs by chemotherapy-induced pain. Symptoms of pain mostly presented during the course of chemotherapy treatment (91.7%), rather than post-treatment, for the 24 participants with CIPN. These symptoms persisted for more than 3 months for 21 out of the 24 participants or 87.5%. Consequently, the pain experienced by participants impacted chemotherapy dosage in subsequent treatments for a large proportion (70.8%)
of the 24 participants with CIPN.
There was a substantial proportion (20.8%) of participants who did not self-report their CIPN symptoms to their physicians. Independent of this, a large proportion (37.5%) of participants did not receive an assessment for their CIPN symptoms from healthcare professionals after their chemotherapy treatment.
Table 2. Participant Pain Presentation
Pain Description |
Frequency |
Prior Chemotherapy (n=68) Yes None |
3(4.4%) 65(95.6%) |
Post Chemotherapy (n=65*) Yes None |
24(36.9%) 41(63.1%) |
SLANSS score (n=24^) <12 >12 |
10(41.7%) 14(58.3%) |
Notes: *: 3 Participants who reported pre-existing pain were excluded from the assessment post-chemotherapy. ^: Only the 24 participants who reported pain post-chemotherapy are included in the SLANSS assessment.
Table 3. Symptoms and Impact of Pain
Characteristics |
Frequency (n=24*) |
Pain on days of least impact No Pain Mild Pain Moderate Pain |
6(25%) 12(50%) 6(25%) |
Pain on days of worst impact No Pain Mild Pain Moderate Pain Severe Pain |
1(4.2%) 3(12.5%) 10(41.7%) 10(41.7%) |
Impact on ADLs None Moderate Severe Life threatening |
10(41.7%) 10(41.7%) 3(12.5%) 1(4.2%) |
Impact on work None Moderate Severe |
17(70.8%) 4(16.7%) 3(12.5%) |
Symptom presentation time During Chemotherapy Post Chemotherapy |
22(91.7%) 2(8.3%) |
Symptom present for >3 months Yes None |
21(87.5%) 3(12.5%) |
Reported to doctor Yes No |
19(79.2%) 5(20.8%) |
Assessed by physician Yes No |
15(62.5%) 9(37.5%) |
Impacted Chemotherapy Dosage Yes No |
17(70.8%) 7(29.2%) |
Notes: *: Only inclusive of participants that reported CIPN
Through binary logistic regression correlation analysis, having a smoking history increased the odds ratio of CIPN by a factor of 3.5 (95% CI: 1.1-11.5) with a statistical significance of p=0.039 (Table 4). Other risk factors such as increasing age, gender (female), radiotherapy and taxane type did not produce a statistically significant correlation with CIPN (p>0.05). However, being female and having a radiotherapy history appeared to have a protective effect against CIPN, producing odds ratios of 0.36 and 0.55 respectively.
Table 4. Correlation Analysis for Risk Factors. Correlation by Binary Logistic Regression between Characteristics and Pain-post-chemotherapy (n=65)
Characteristic |
Odds ratio [95% CI] |
p-value |
Age |
0.98 [0.93,1.02] |
0.34 |
Gender (female) |
0.36 [0.08,1.64] |
0.19 |
Smoking history |
3.51 [1.07,11.53] |
0.04 |
Radiotherapy history |
0.55 [0.17,1.76] |
0.32 |
4 DISCUSSION
This prospective cohort study found an incidence rate of 36.9% for chemotherapy-induced peripheral neuropathy in the primary analysis, amongst 65 Australian participants who had undergone taxane-based chemotherapy. A significant proportion of these participants (58.3%) also reported a score of more than 12 on the S-LANSS assessment scale. These findings are supportive of results in previous literature, where incidence rates of taxane-induced peripheral neuropathy varied from 13% to 62%[5].
Studies have shown limited effective treatment options for patients suffering from CIPN and the most common preventative approaches are to reduce chemotherapy dosages[12]. In this study, the painful symptoms of CIPN were also demonstrated to impact subsequent dosages of chemotherapy, with a large proportion (70.8%) of participants with CIPN had their chemotherapy dosages either reduced or ceased completely (Table 3). Early cessation of therapy can be detrimental to patients’ cancer survivability as well as mental health. Patients who have premature termination or dosage reduction in their chemotherapy can not only suffer from the possibility of cancer remission but also experience anxiety about their future prognosis. This is then likely to negatively impact participants’ QoL.
The ADLs, and subsequently the QoL, of more than 50% of participants with CIPN were impacted by the complications of pain. This result highlights the severity of CIPN, given the harsh consequences that some patients experience for an extended period of time. In this study, 87.5% of participants with CIPN were still experiencing symptoms for more than three months. This duration of effect on patients’ quality of life is similar to that seen in other, more well-studied, chronic pain conditions such as arthritis and chronic back pain[13]. Thus, the impact of CIPN on quality of life can similarly become severe for a large population of patients with CIPN.
Additionally, it was found that 20.8% of participants with CIPN did not self-report their symptoms to their physicians. This could have implications for their recovery as therapy options cannot be provided efficiently if there is a delay in diagnosis. A contributing factor to this could be a failure in patient education on the potential signs and symptoms of CIPN. To improve awareness in the future, better education could be provided to patients on the common symptoms of CIPN and patients should be more strongly encouraged to self-report these as early as possible, if they arise. Independent to patient reporting, 37.5% of participants with CIPN believed that they did not receive an assessment of their CIPN symptoms post-chemotherapy from any clinician. This raises the question of whether there is a need for more training for clinicians on CIPN symptoms as well as better assessment tools. Potential future studies could explore these issues with a view to improve the rates of early diagnosis and assessment of CIPN.
This study found a significant correlation between taxane-based CIPN and those with a smoking history (p=0.039). Tobacco is well known for its carcinogens and smoking has significant impacts on overall health. Smoking is also a common risk for other types of peripheral neuropathy such as diabetes[14], as well as Cisplatin-based CIPN[15]. However, as the molecular mechanisms of CIPN are still unclear, few studies have been conducted on the exact pathway through which smoking may affect the emergence of symptoms. Studies have shown and postulated that the association may be a result of reduced peripheral blood flow, a consequence of long-term smoking[16]. Future research should investigate whether smoking has a causation effect on taxane-based CIPN as well as the pathophysiology of this association.
The strengths of this prospective cohort study include consistent data collection for all participants, a validated definition of outcome measures, and the ability to assess longitudinal factors. Having a validated assessment tool is important for the reliability of the data as the condition is complex and it may be difficult to differentiate symptoms from other factors without one. This study used a validated assessment and was able to assess each patient more accurately. However, the study was also limited by its small sample size and possible sampling variability as data originated from a single centre. As a result, some secondary outcome measures of this study were underpowered. A larger sample size would reduce variability and allow more accurate estimations of risk factor correlation. Additionally, the assessment criteria and results of this study were reliant on self-reported data from participants. Although the assessment tools used were validated for the signs and symptoms of CIPN, the scale of symptoms of pain is subjective to the individual. Other limitations of this study were possible confounding factors that could not be controlled such as demographic characteristics, co-morbidities, the use of concurrent therapeutics, and cumulative drug dosage.
5 CONCLUSION
This study shows that there is a large proportion of Australian patients undergoing taxane-based chemotherapy who are experiencing CIPN and many of whom live with these painful symptoms chronically. Smoking is also found to be a risk factor for CIPN. Obtaining an understanding of risk factors is useful for the education of both physicians and patients as well as the introduction of possible preventative methods. Future research should explore prevention and therapeutic options for patients with a higher risk of CIPN.
Acknowledgements
The researchers would like to thank Dr. Tim Hucker for assistance in project planning; thank Dr. Nick Smoll for technical help; thank Dr. Marlise Alexander for pharmacy support and access to records.
Conflicts of Interest
There are no conflicts of interests that the researchers need to declare. The data that support the findings of this study are available on request from the corresponding author.
Author Contribution
Ms Ciara Power – Formulating and proposing the research idea; data collection and supervision of article write-up
Dr Jamie Young – Supervision of article write-up
Ms Xinqi Liu – Data analysis and article write-up and revision
Ms Diana Munteanu – Data collection
Abbreviation List
ADLs: Activities of daily living
BMI: Body mass index
CIPN: Chemotherapy-induced peripheral neuropathy
CTCAE: Common terminology criteria for adverse events
OR: Odds Ratios
QoL: Quality of life
S-LANSS: Self-reported Leeds Assessment of Neuropathic Symptoms and Signs
TIPN: Taxane-induced peripheral neuropathy
References
[1] Quasthoff S, Hartung HP. Chemotherapy-induced peripheral neuropathy. Journal of neurology, 2002; 249: 9-17.[DOI]
[2] Starobova H, Vetter I. Pathophysiology of chemotherapy-induced peripheral neuropathy. Frontiers in molecular neuroscience, 2017; 10: 174.[DOI]
[3] Zajączkowska R, Kocot-Kępska M, Leppert W et al. Mechanisms of chemotherapy-induced peripheral neuropathy. International journal of molecular sciences, 2019; 20: 1451.[DOI]
[4] da Costa R, Passos GF, Quintão NLM et al. Taxane‐induced neurotoxicity: Pathophysiology and therapeutic perspectives. British journal of pharmacology, 2020; 177: 3127-3146.[DOI]
[5] Burgess J, Ferdousi M, Gosal D et al. Chemotherapy-induced peripheral neuropathy: epidemiology, pathomechanisms and treatment. Oncology and therapy, 2021: 1-66.
[6] Starobova H, Vetter I. Pathophysiology of chemotherapy-induced peripheral neuropathy. Frontiers in molecular neuroscience, 2017; 10: 174.[DOI]
[7] Shah A, Hoffman EM, Mauermann ML et al. Incidence and disease burden of chemotherapy-induced peripheral neuropathy in a population-based cohort. Journal of Neurology, Neurosurgery & Psychiatry, 2018; 89: 636-641.[DOI]
[8] Bonhof CS, Mols F, Vos MC et al. Course of chemotherapy-induced peripheral neuropathy and its impact on health-related quality of life among ovarian cancer patients: a longitudinal study. Gynecologic oncology, 2018; 149: 455-463.[DOI]
[9] Zanville NR, Nudelman KNH, Smith DJ et al. Evaluating the impact of chemotherapy-induced peripheral neuropathy symptoms (CIPN-sx) on perceived ability to work in breast cancer survivors during the first year post-treatment. Supportive Care in Cancer, 2016; 24: 4779-4789.[DOI]
[10] Molassiotis A, Cheng HL, Leung KT et al. Risk factors for chemotherapy‐induced peripheral neuropathy in patients receiving taxane‐and platinum‐based chemotherapy. Brain and behavior, 2019; 9: e01312.[DOI]
[11] Herrero Babiloni A, Nixdorf DR, Law AS et al. Initial accuracy assessment of the modified S-LANSS for the detection of neuropathic orofacial pain conditions. Quintessence International, 2017; 48.
[12] Flatters SJL, Dougherty PM, Colvin LA. Clinical and preclinical perspectives on Chemotherapy-Induced Peripheral Neuropathy (CIPN): a narrative review. BJA: British Journal of Anaesthesia, 2017; 119: 737-749.[DOI]
[13] Husky MM, Ferdous Farin F, Compagnone P et al. Chronic back pain and its association with quality of life in a large French population survey. Health and quality of life outcomes, 2018; 16: 1-9.[DOI]
[14] Su S, Wang W, Sun T et al. Smoking as a risk factor for diabetic nephropathy: a meta-analysis. International urology and nephrology, 2017; 49: 1801-1807.[DOI]
[15] Dolan ME, El Charif O, Wheeler HE, et al. Clinical and genome-wide analysis of cisplatin-induced peripheral neuropathy in survivors of adult-onset cancer. Clinical Cancer Research, 2017; 23: 5757-5768.[DOI]
[16] Kawakami K, Tunoda T, Takiguchi T, et al. Factors exacerbating peripheral neuropathy induced by paclitaxel plus carboplatin in non-small cell lung cancer. Oncology research, 2012; 20: 179-185.[DOI]
Copyright © 2024 The Author(s). This open-access article is licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, sharing, adaptation, distribution, and reproduction in any medium, provided the original work is properly cited.


