Effect of Recombinant Human Adenovirus Type 5 Injection Combined with Haploidentical Natural Killer Cell Immunotherapy on Immune Function and Adverse Reactions in Patients with Malignant Ascites Caused by Ovarian Cancer
Lan Pang1, Yan Li1, Dongxia Sun1*
1Department of gynaecology, Handan Maternal and Child Health Care Hospital, Hebei Province, China
*Correspondence to: Dongxia Sun, Department of Gynaecology, Handan Maternal and Child Health Care Hospital, Handan 056001, Hebei Province, China; Email: Sundognxia120@163.com
Abstract
Objective: To explore the effect of recombinant human adenovirus type 5 injection combined with haploidentical natural killer cell immunotherapy on immune function and adverse reactions in patients with malignant ascites caused by ovarian cancer (OC).
Methods: From January 2018 to September 2019, 65 patients with advanced OC combined with malignant ascites who received treatment in the oncology department of our hospital were collected. According to the treatment methods, the patients were assigned to study group (SG) (35 cases) and control group (CG) (30 cases). In CG, patients were treated with NK cell reinfusion. SG: On the basis of the CG, the recombinant human adenovirus type 5 injection was injected directly into tumour. The peripheral blood mononuclear cells of lineal relatives of all patients were cultivated by antibody coating and co-stimulation with various cytokines, and the NK cells cultured in vitro were returned to the patients for infusion twice on the 14th and 15th days, respectively. The clinical efficacy, changes of serum tumour markers, changes of immune function indicators and adverse effects were compared between the two groups.
Results: The objective remission rate of clinical efficacy in the SG was obviously higher than that in the CG. Before therapy, the levels of serum carcinoembryonic antigen, carbohydrate antigen 242, carbohydrate antigen 19-9, alpha-fetoprotein and neuron specific enolase had no statistically significant difference in both groups (P>0.05). After therapy, the level of each index in the SG was better than that in the CG, with statistically significant difference (P<0.05). After therapy, the levels of peripheral NK cells, CD4+/CD8+ ratio, CD3+CD4+ and CD3+ level in SG were obviously higher than those before treatment, while the levels of CD4+CD25+ were obviously lower than those before treatment, and the indexes in the SG were obviously better than those in the CG (P<0.05). Before therapy, there was no obvious difference in quality of life between the two groups. After treatment, the overall quality of life in the SG was higher than that in the CG, with statistically significant difference (P<0.05). The incidence of hepatic and renal insufficiency had no statistically significant difference between SG and CG (P>0.05). However, the incidence of nausea, vomiting, abdominal pain and diarrhea in the SG was obviously lower than that in the CG, with statistically significant difference (P<0.05).
Conclusion: Recombinant human adenovirus type 5 injection combined with haploidentical natural killer cell immunotherapy can better recover the immune function and reduce the incidence of adverse reactions in patients with malignant ascites caused by OC.
Keywords: recombinant human adenovirus type 5 injection, haploidentical natural killer cell, immunotherapy, OC, malignant ascites, immunologic function
1 INTRODUCTION
Ovarian cancer (OC) is a common malignant tumour of female reproductive system in clinic. At present, its incidence is second only to that of cervical carcinoma and corpus carcinoma, and its prognosis is poor[1]. In recent years, the incidence rate is rising year by year[2]. Ovarian tumour is a heterogeneous tumour, including epithelial tumour[3], germ cell tumour[4], sex cord stromal tumour[5] and stromal tumour[6]. Approximately 90%-95% of all patients belong to epithelial tumors[7]. According to the latest classification published by World Health Organization (WHO)[8], it is divided into serous carcinoma, mucinous carcinoma, serous mucinous carcinoma, endometrioid adenocarcinoma, clear cell carcinoma, brenner tumour and undifferentiated carcinoma. Most patients with OC are confirmed at an advanced stage, so they have lost the opportunity of surgical treatment. Patients with advanced OC will be complicated with a large number of ascites, which leads to poor clinical efficacy, poor prognosis and easy recurrence, so the survival rate of clinical OC is relatively low.
Malignant ascites usually develops in the progression of certain types of cancer, such as OC[9] and pancreatic carcinoma[10]. These exudates contain a large number of tumour cells and they are metastatic[11]. These patients usually have a large amount of peritoneal effusion (usually several liters). The acellular part of malignant pleural effusion is rich in cytokines, chemokines, growth factors and extracellular matrix components[12]. In addition to tumour cells, the effusion also contains a large number of non-malignant cells and various immune cells, including macrophages and lymphocytes[13]. At present, the clinically recognized treatment methods for these solid tumours mainly include drug therapy, surgery, chemoradiotherapy and palliative treatment that aims to improve the quality of life of patients[14]. These treatments can alleviate the disease to a certain extent, but there are still some problems, such as low cure rate, drug resistance, tumour recurrence and immunity reduction caused by radiotherapy and chemotherapy. Studies have revealed that the demonstrated of tumors are closely bound up with the immune status of patients, and natural killer cells play a crucial role in the immune surveillance of tumours[15]. Since 1995[16], many international organizations have carried out clinical research on the application of autologous or allogeneic NK cells. Recombinant human adenovirus type 5[17] is an oncolytic virus, which is obtained by modifying human adenovirus through gene recombination technology, and the modified adenovirus can selectively proliferate and replicate in large quantities in human tumour cells, thus killing tumour cells. This research was mainly designed to observe the effects of recombinant human adenovirus type 5 injection combined with haploidentical natural killer cell immunotherapy on the improvement of immune function and adverse reactions in patients with malignant ascites casued by OC, which are reported as below.
2 MATERIALS AND METHODS
2.1 Research Objects
From January 2018 to September 2019, 65 patients with advanced OC comorbid with malignant ascites who received treatment in the oncology department of our hospital were collected. According to the treatment methods, they were divided into study group (SG) and control group (CG). There were 35 cases in the SG, aged 51-79 years old. There were 30 cases in the CG, aged 53-80 years old.
Inclusion criteria: All patients were diagnosed with OC by pathological diagnosis; Through the cytological examination of ascites, the patient was confirmed to have ascites caused by peritoneal metastasis of OC; By ultrasound examination, the patient was confirmed to have more than a moderate amount of ascites; Before treatment, patients did not receive anti-tumor therapy for 4 weeks or more; The blood routine, liver and kidney function, blood coagulation index and electrocardiogram were normal; The KPS score of patients' physical condition was ≥70.
Exclusion criteria were as follows: severe anemia and malnutrition; accompanied by malignant tumors in other parts; serious liver and kidney function diseases; severe infection.
In addition, all the immediate family members of healthy cancer patients (aged 18-45) were selected as donors of natural killer cell. The general data of patients in the two groups are displayed in Table 1, showing that the basic characteristics of patients had no statistically significant difference (P<0.05), which was comparable. This research has been ratified by the Ethics Committee of our hospital, and all patients have affixed informed consent.
Table 1. Characteristic of the SG and CG
|
SG (n=35) |
CG (n=30) |
χ2/t |
P |
Age/Years Old |
56.1±8.5 |
55.7±7.9 |
0.0808 |
0.9361 |
Bmi (kg/m2) |
22.4±2.1 |
23.1±2.0 |
0.5761 |
0.5687 |
Figo Staging |
|
|
0.5191 |
0.4712 |
Stage Iii |
24 (68.6) |
18 (60.0) |
|
|
Stage Iv |
11 (31.4) |
12 (40.0) |
|
|
Pathological Types |
|
|
0.7861 |
0.9403 |
Serous Adenocarcinoma |
22 (62.8) |
21 (70.0) |
|
|
Mucinous Adenocarcinoma |
4 (11.4) |
3 (10.0) |
|
|
Endometrioid Adenocarcinoma |
4 (11.4) |
2 (6.7) |
|
|
Undifferentiated Carcinoma |
3 (8.6) |
3 (10.0) |
|
|
Clear Cell Carcinoma |
2 (5.8) |
1 (3.3) |
|
|
Kps Score |
74.6±3.4 |
75.2±3.1 |
0.3176 |
0.7529 |
Migration Type |
|
|
0.7979 |
0.9387 |
Pulmonary Metastasis |
9 (25.7) |
6 (20.0) |
|
|
Lymph Node Metastasis |
12 (34.3) |
9 (30.0) |
|
|
Hepatic Metastasis |
8 (22.8) |
8 (26.7) |
|
|
Osseous Metastasis |
6(17.2) |
7 (23.3) |
|
|
2.2 Methods of Treatment
All patients were routinely subjected to peritoneal puncture and catheterization, and the ascites was drained first. When there was a large amount of ascites, it could not be drained clean at a time to avoid hypotension and shock. After the ascites was drained clean, patients in CG received NK cell reinfusion once a day for 2 days, and 21 days was a cycle. SG: On the basis of the CG, recombinant human adenovirus type 5 injection was injected directly into tumour, once a day, continuously for 5 days and 21 days as a cycle. According to the tumour size, the injection dose was adjusted from 5.0×1011vp/d (one) to 1.5×1012 vp/d (three).
2.3 Preparation of Natural Killed Cells
The 80mL of peripheral venous blood (10mL for detection +70mL for culture and amplification of immune cells) was drawn from donors in each group, which was applied for testing. The blood was centrifuged to separate the serum and inactivated at 56℃ for 1h. The peripheral blood mononuclear cells (PBMC) were obtained from the remaining blood samples with lymphocyte separation solution, and then resuspended in serum-free cell culture media. The cell density was changed to 1-2×106/mL in the cell culture flask, and NK cell activator coating was added. The IL-15, IL-2 and autogenous plasma were added at the final concentration of 50ng/mL, 1000U/mL and 5% respectively, and cultivated in a cell incubator at 37 ℃, 5% CO2 and saturated humidity. Every 2-3 days, the cell state was observed and tested, and the cytokines and serum-free medium were added according to the initial culture concentration. Then, they were cultivated for 14-15 days. NK cells were collected after passing the inspection by the clinical examination center of the hospital, and the cell viability and function were counted and tested. After passing the quality inspection, the cells were resuspended with 100mL of physiological saline comprising 5% human albumin, and the corresponding NK cell samples were kept in storage.
2.4 Detection of NK Cell Phenotype
The cell phenotype was stained with fluorescent labeled monoclonal antibody. The 1×106 cells or whole blood (300µl) were added to each reaction tube, and T cell subgroup detection antibody was added (tube 1: CD3 FITC, CD45PerCP-Cy5.5, CD4 APC, CD8 PE; tube 2: CD3 FITC, CD45PerCP-Cy5.5, CD19 APC, CD16CD56 PE). The corresponding isotype control antibody was added to the negative control tube and acted in dark at 4ºC for 30min (if it was whole blood, the red blood cell lysis buffer were added and centrifuged to remove the supernatant). After washing with PBS for 2 times, the paraformaldehyde (1g/L) was added again for fixation, and then stored at 4ºC away from light. The machine detection was conducted within 24h. The cell ratio of CD16+CD56+ was >80% and CD3-CD16+CD56+ cell > was 50%.
2.5 Cell Infusion Protocol
On the 14th and 15th day of culture, NK cells were pretreated with 100mL of 5% glucose injection. Then, the patients were injected intravenously and slowly to establish intravenous channels, and the infusion was done at a slow speed within 10min of the cell refusion. After patients had no adverse reactions, NK cells were slowly infused at normal speed. The concentration of reinfusion cells was not higher than 5×107/mL, and the infusion rate was no more than 50 drops per minute. To prevent cell deposition, the cell suspension was mixed upside down once every 10min in the process of reinfusion, and then the pipeline was flushed with 100mL of normal saline after the completion of reinfusion. The whole reinfusion process was closely monitored. Doctors and nurses observed and recorded the reaction of patients throughout the course. The patients received direct intravenous infusion through blood transfusion apparatus, and the reinfusion dose was 0.5-2.5×109/time.
2.6 Evaluation of Clinical Efficacy
According to the WHO evaluation criteria for the efficacy of ascites: Complete remission (CR): the ascites disappeared completely lasted for more than one month; Partial remission (PR): the volume of ascites was reduced by more than half compared with that before treatment and maintained for more than 1 month; Stable disease (SD): the volume of ascites did not increase or decrease obviously, which lasted for more than one month; Progressive disease (PD): the amount of ascites increased obviously compared with that before treatment. Objective response rate =(CR+PR) cases/total cases ×100%.
The levels of serum tumour markers carbohydrate antigen 19-9 (CA19-9), alpha-fetoprotein (AFP), neuron specific enolase (NSE), carcinoembryonic antigen (CEA) and carbohydrate antigen 242 (CA242) were detected and compared between the two groups before and after treatment. The fasting venous blood (10mL) was drawn before and after treatment, and the blood was centrifuged at 3000r/min for 20min to separate the serum. The supernatant was obtained to be measured, and the levels of tumour markers in serum were tested via enzyme-linked immunosorbent assay.
Detection of related indexes of immune function: The peripheral venous blood (3mL) was drawn in the morning before and after treatment, and the relevant indexes of T cell subgroup were detected by fluorescence antibody method. It included CD3+, CD3+CD4+, CD4+/CD8+, CD4+CD25+ and NK cells.
Quality of life score: The SF-36 quality of life evaluation scale was applied, which mainly included overall health, vitality, physical function, role physical, physical pain, emotional role, social function and psychical health. The higher the score, the better the patient's quality of life.
The adverse reactions were evaluated according to the WHO 5-level grading standard for adverse reactions: Grade 0 meant no adverse reactions; Grade 1 meant slight adverse reactions; Grade 2 meant medium adverse reactions; Grade 3 meant serious adverse reactions; Grade 4 meant severe complications. In this research, grade 0-1 adverse reactions were classified as no or slight adverse reactions, and grade 2-4 adverse reactions were classified as moderate and severe adverse reactions.
2.7 Statistical Methods
SPSS22.0 was used to process the data. The quantitative data were represented by the mean number ± standard deviation (x±s). Paired t-test was used for comparison within groups before and after therapy. Independent sample T test was used for comparison between groups. The counting data were represented as a case (%). χ2 test was applied for comparison between groups. The difference was statistically significant with P<0.05.
3 RESULTS
3.1 Expansion and Quality Control Chart of Natural Killer Cells In Vitro
It could be concluded from Figure 1A that the frequency of NK cells reached 65.8% on the 8th day, 77.8% on the 14th day and 82.9% on the 15th day after culture. The expression level of CD56 molecule was different, and NK cells could be assigned to two subgroups: CD56 bright NK cells and CD56 dim NK cells. The main function of CD56 dim NK cells was to kill target cells directly, while CD56 bright NK cells had strong cytokine secretion ability, which could play an immunomodulatory role by secreting cytokines. From Figure 1B, we could found that the NK cells of donor changed from highly expressing CD56 dim to highly expressing CD56 bright after cell culture for 14 days. It could be concluded from Figure 1C and 1D that the total cell number and NK cell number were multiplied. CD3-CD15+CD56+NKT cells were another important anti-tumour effector cells, which played an active role in the process of cellular immunotherapy. In this research, CD3-CD15+CD56+NKT cells accounted for a large proportion besides NK cells after culture and expansion for 15 days (Figure 1E).
|
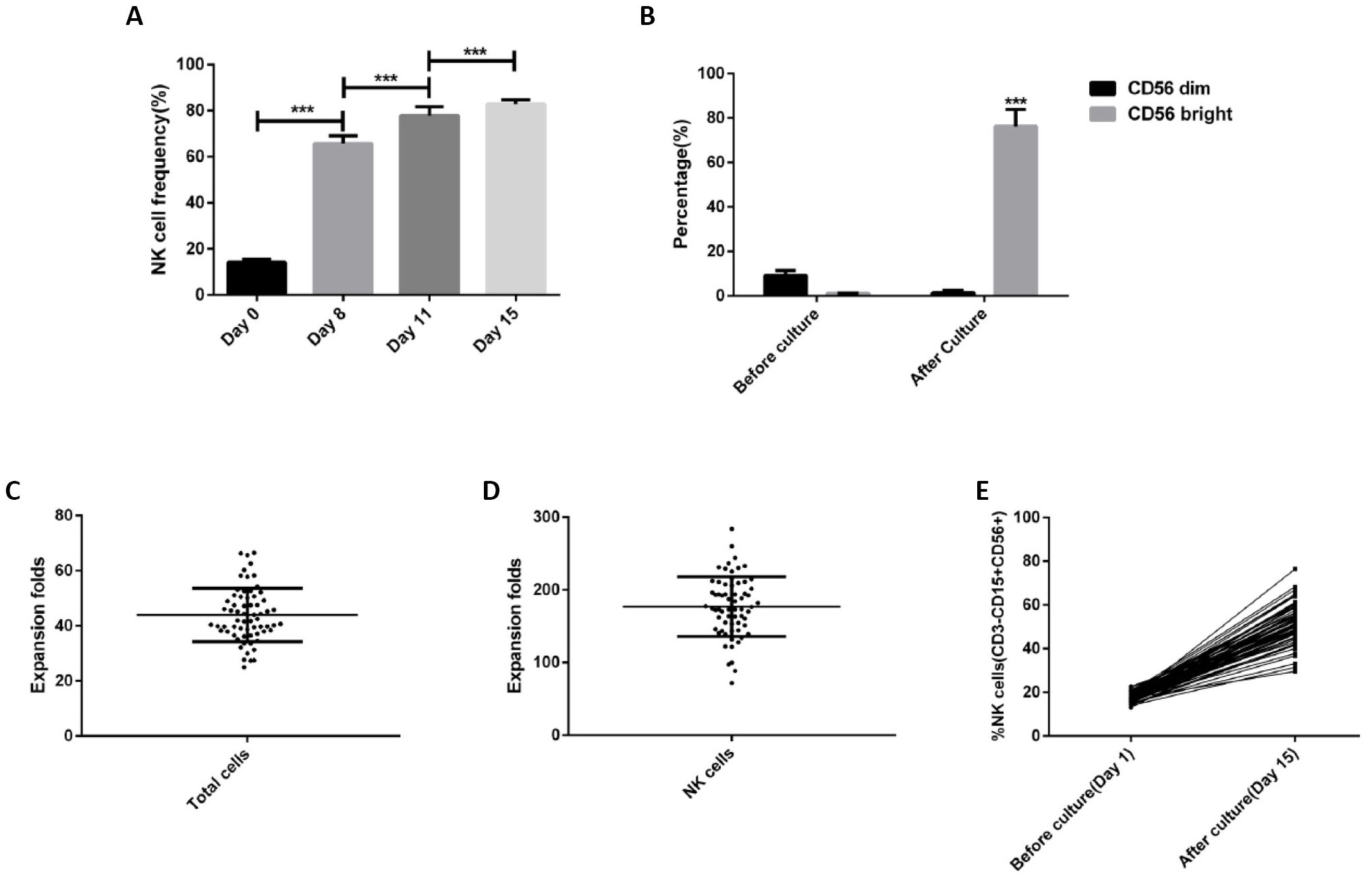
Figure 1. Expansion and quality control chart of natural killer cells in vitro. A: Typical graph of NK cell frequency changing with culture time; B: Changes of NK cell subsets before and after culture; C: Amplification multiples of all immune cells; D: Amplification multiples of NK cell; E: Quality control of NK cells before and after culture; ***meant that compared with that before culture, P<0.001.
3.2 Comparison of Clinical Curative Effect between the Two Groups
The objective response rate in the SG was 60.0% (21/35), which was higher than that in the CG (33.3%, 10/30), with statistically significant difference (P<0.05) (Table 2).
Table 2. Comparison of Clinical Efficacy between the Two Groups
|
CR |
PR |
SD |
PD |
Objective Response Rate |
CG (n=30) |
4 (13.3) |
6 (20.0) |
11 (36.7) |
9 (30.0) |
10 (33.3) |
SG (n=35) |
7 (20.0) |
14 (40.0) |
10 (28.6) |
4 (11.4) |
21 (60.0) |
χ2/t |
|
|
|
|
4.6051 |
P |
|
|
|
|
0.0319 |
3.3 Comparison of Serum Tumour Markers between the Two Groups before and after Therapy
Before therapy, the levels of serum CEA, CA242, CA19-9, AFP and NSE had no statistically significant difference in both groups (P>0.05). After therapy, the levels of all indexes decreased, and the level of patients in the SG was better than that in the CG, with statistically significant difference (P<0.05).
|
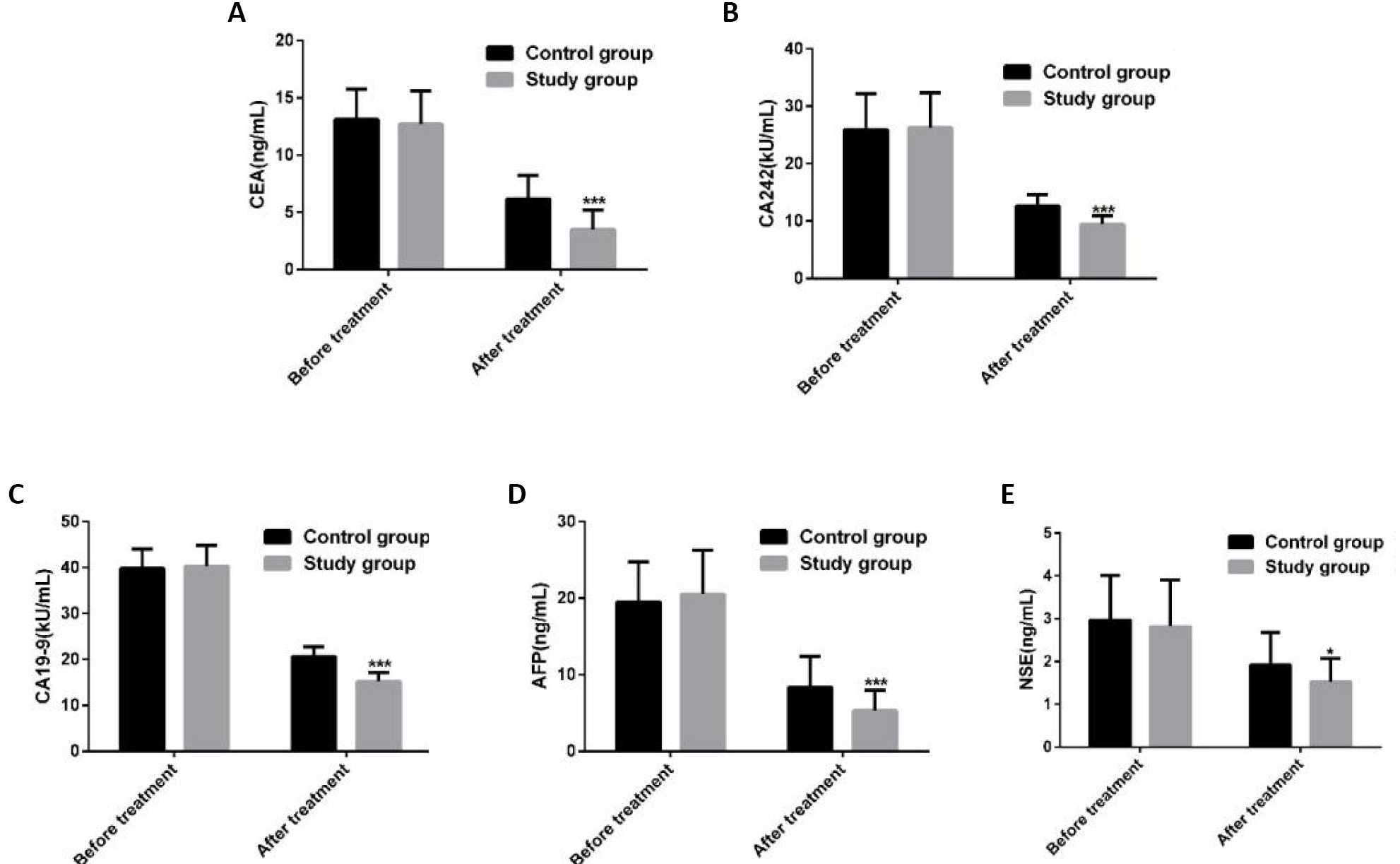
Figure 2. Comparison of serum tumour markers between the two groups before and after treatment. A: Serum CEA level of patients in both groups before and after treatment; B: Serum CA242 levels of patients in both groups before and after treatment; C: Serum CA19-9 levels of patients in both groups before and after treatment; D: Serum AFP levels of patients in both groups before and after treatment; E: Serum NSE levels of patients in both groups before and after treatment.
3.4 Comparison of Immune Function Indexes between the Two Groups before and after Therapy
Before therapy, there was no obvious difference in peripheral CD4+CD25+, NK cells, CD4+/CD8+ ratio, CD3+CD4+, CD3+ levels in both groups (P>0.05). After therapy, the levels of peripheral NK cells, CD4+/CD8+ ratio, CD3+CD4+ and CD3+ in the observation group were obviously higher than those before treatment, and the SG was markedly higher than the CG (P<0.05). The CD4+CD25+ was obviously lower than that before treatment, but the SG was higher than the CG (P<0.05) (Table 3).
Table 3. Immune Function Indexes in Both Groups before and after Treatment
|
CD4+CD25+ (%) |
CD4+/CD8+ (%) |
CD3+CD4+ (%) |
CD3+ (%) |
NK Cells (%) |
|
Before Treatment |
CG (n=30) |
12.56±2.05 |
1.01±0.15 |
29.12±5.26 |
50.02±4.26 |
13.41±1.42 |
SG (n=35) |
11.58±2.13 |
1.02±0.16 |
30.53±5.86 |
51.15±5.87 |
13.81±1.54 |
|
χ2/t |
1.8814 |
0.2585 |
1.0134 |
0.8748 |
1.0819 |
|
P |
0.0645 |
0.7968 |
0.3147 |
0.3849 |
0.2834 |
|
After Treatment |
CG (n=30) |
8.23±2.87 |
1.08±0.13 |
30.51±4.26 |
51.69±3.01 |
15.03±3.68 |
SG (n=35) |
10.64±3.41 |
1.38±0.20 |
42.35±5.01 |
62.15±6.11 |
24.58±4.02 |
|
χ2/t |
3.0528 |
7.0361 |
10.1688 |
8.5252 |
9.9253 |
|
P |
0.0033 |
<0.0001 |
<0.0001 |
<0.0001 |
<0.0001 |
|
3.5 Comparison of Quality of Life between the Two Groups
Before treatment, there was no obvious difference in indexes of quality of life in both groups (P>0.05). After therapy, the scores of quality of life in both groups were improved, and the scores of SG were obviously higher than that of CG in terms of overall health, physiological function, physiological role, physical pain and vitality, with statistically significant difference (P<0.05). Nevertheless, the emotional function, social function, mental health and general health had no statistically significant difference in both groups (P>0.05) (Table 4).
Table 4. Quality of Life Scores in Both Groups before and after Treatment
|
Before Treatment |
After Treatment |
||||||
CG (n=30) |
SG (n=35) |
χ2/t |
P |
CG (n=30) |
SG (n=35) |
χ2/t |
P |
|
Overall Health |
47.81±4.91 |
48.62±5.03 |
0.6544 |
0.5152 |
56.36±6.02 |
65.28±6.78 |
5.5658 |
<0.0001 |
Physiological Function |
51.26±5.36 |
52.26±5.68 |
0.7261 |
0.4704 |
57.63±6.81 |
68.34±7.07 |
6.1922 |
<0.0001 |
Physiological Role |
53.26±6.38 |
54.58±6.82 |
0.8012 |
0.4259 |
61.52±6.28 |
70.36±7.36 |
5.1612 |
<0.0001 |
Emotional Function |
73.15±7.43 |
74.68±7.91 |
0.7994 |
0.4271 |
77.62±7.51 |
78.03±7.26 |
0.2234 |
0.8239 |
Social Function |
38.35±4.18 |
39.25±4.05 |
0.8800 |
0.3822 |
46.84±4.26 |
47.35±4.82 |
0.4485 |
0.6553 |
Physical Pain |
46.63±5.69 |
47.62±6.03 |
0.6771 |
0.5008 |
55.25±5.68 |
63.58±6.79 |
5.3114 |
<0.0001 |
Vitality |
57.26±5.02 |
58.68±5.61 |
1.0674 |
0.2898 |
66.38±6.91 |
79.02±8.02 |
6.7472 |
<0.0001 |
Mental Health |
64.28±7.09 |
65.26±7.38 |
0.5434 |
0.8557 |
71.25±7.82 |
72.65±8.36 |
0.6933 |
0.4907 |
General Health |
68.25±6.92 |
69.36±7.01 |
0.6402 |
0.5244 |
72.36±7.68 |
73.67±7.97 |
0.6718 |
0.5041 |
3.6 Comparison of the Incidence of Adverse Reactions between the Two Groups
The incidence of hepatic and renal insufficiency had no statistically significant difference between the SG and the CG (P>0.05). However, the incidence rate of nausea, vomiting, abdominal pain and diarrhea in SG was obviously lower than that in CG, with statistically significant difference (P<0.05) (Table 5).
Table 5. Incidence of Adverse Reactions in Both Groups
|
Nausea and Vomiting |
Abdominal Pain |
Diarrhea |
Hepatic Insufficiency |
Renal Insufficiency |
|
CG (n=30) |
Grade 0-1 |
12 (40.0) |
16 (53.3) |
15 (50.0) |
10 (33.3) |
9 (30.0) |
Grade 2-4 |
18 (60.0) |
14 (46.7) |
15 (50.0) |
20 (66.7) |
21 (70.0) |
|
SG (n=35) |
Grade 0-1 |
24 (68.6) |
28 (80.0) |
30 (85.7) |
19 (54.3) |
17 (48.6) |
Grade 2-4 |
11 (31.4) |
7 (20.0) |
5 (14.3) |
16 (45.7) |
18 (51.4) |
|
χ2/t |
5.3371 |
5.2531 |
9.6731 |
2.8701 |
2.3211 |
|
P |
0.0209 |
0.0219 |
0.0019 |
0.0902 |
0.1276 |
|
4 DISCUSSION
Natural killer cells are a new lymphocyte subgroup except T cells and B cells, which were discovered in 1973. It is named for its ability to kill tumor cells without specific antigen receptor[18]. Based on CD56 and CD16, the human NK cells can be assigned to two subgroups: CD56 dim and CD56 bright. CD56 dim NK cells mostly exist in peripheral blood, while CD56 bright NK cells mainly function in tissues and secondary lymphoid organs[19]. Now researchers generally believe that CD56 bright NK cells have stronger cytokine secretion ability and immune regulation function, which can regulate natural immunity and specific immune response, and have certain cytotoxicity under some stimulation conditions[20]. CD56 bright NK cells play a vital role in infection, inflammation, autoimmune diseases and tumours[21]. Recombinant human adenovirus type 5 (H101) is a genetically engineered adenovirus that lacks Elb55ku protein. The tumour cells with mutant P53 are infected with H101, and then they can replicate and play an oncolytic role in tumour cells due to loss of P53 protein function. After cell death, the virus released infects the surrounding tumour cells and further kills the tumour. It has been reported[22] that the modified recombinant human adenovirus type 5 (H101) can kill tumour cells, but the damage to healthy human cells is minimal.
The results of this research revealed that the objective response rate of SG was higher than that of CG, which indicated that the therapeutic effect of recombinant human adenovirus type 5 injection combined with haploidentical natural killer cell immunotherapy for malignant ascites caused by OC was better than that of single natural killer cell immunotherapy. The results also revealed that the changes of tumour marker levels were also analyzed before and after therapy. Before therapy, the serum CEA, CA242, CA19-9, AFP and NSE levels had no statistically significant difference in both groups (P>0.05). After therapy, the level of each indicator in the SG was obviously better than that in the CG. CEA is an acid glycoprotein with human embryonic antigen characteristics, which exists on the surface of tumour cells differentiated from endoderm cells, and it is a constitutive protein of cytomembrane, and belongs to a broad-spectrum tumour marker[23]. CA242, an early indicator for detection of OC, has a higher positive rate in serous cystadenocarcinoma of the ovary, and it will also increase to varying degrees in patients with benign ovarian epithelial tumors and uterine fibroids[24]. CA19-9 is a mucin glycoprotein antigen, which is mainly expressed by malignant tumour mucin, so the positive rate is higher in ovarian mucinous carcinoma[25]. AFP is a glycoprotein, which can be applied as a positive testing index for various tumours[26]. NSE is an acid protease peculiar to neurons and neuroendocrine cells. It is a specific marker of neuroendocrine tumors and can be applied for differential diagnosis, disease monitoring, efficacy evaluation and recurrence prediction[27]. After treatment, the levels of peripheral NK cells, CD4+/CD8+ ratio, CD3+CD4+ and CD3+ level in the SG were obviously higher than those before treatment, while the levels of CD4+CD25+ were obviously lower than those before treatment, and the indexes in the SG were obviously better than those in the CG. In the process of cellular immunity, T lymphocytes and NK cells play a vital role in immune regulation[28]. The number of NK cells decreases with the growth of tumour cells. CD3+ can reflect the total number of mature T lymphocytes. CD4+, as an auxiliary T cell, is the main member of the body's anti-tumour immunity. The ratio of CD4+/CD8+ can predict the killing ability of patient’s body to tumour cells[29]. The results showed that cell immunotherapy could combine with target cells to play a direct killing role, and it could produce a large number of cytokines, thus achieving the purpose of indirectly killing tumors and inducing apoptosis and necrosis of tumour cells. In addition, the overall quality of life in the SG after treatment was better than that in the CG, and the incidence of adverse reactions was also lower than that in the CG, with statistically significant difference. The results showed that recombinant human adenovirus type 5 injection combined with natural killer cell immunotherapy had higher safety.
5 CONCLUSION
To sum up, recombinant human adenovirus type 5 injection combined with haploidentical natural killer cell immunotherapy can improve the immune function of patients with malignant ascites caused by OC, improve their quality of life, and reduce the incidence of adverse reactions after treatment, with higher safety. Because the sample size of this research is small, the long-term effect needs to be further observed. Next, we will increase follow-up to track the prognosis.
Acknowledgments
Not applicable.
Conflicts of Interest
These authors declared no conflict of interest.
Author Contribution
Sun D designed this study and wrote the article; Pang L and Li Y collected the data, performed the statistical analysis, and revised the papers for important intellectual content; all authors approved the final version.
Abbreviation List
AFP, Alpha-fetoprotein
CA19-9, Carbohydrate antigen 19-9
CA242, Carbohydrate antigen 242
CEA, Carcinoembryonic antigen
CG, Control group
CR, Complete remission
NSE, Neuron specific enolase
OC, Ovarian cancer
SD, Stable disease
SG, Study group
PD, Progressive disease
PR, Partial remission
References
[1] Stewart C, Ralyea C, Lockwood S. Ovarian cancer: An integrated review. Semin Oncol Nurs, 2019; 35: 151-156. DOI: 10.1016/j.soncn.2019.02.001
[2] Webb PM, Jordan SJ. Epidemiology of epithelial ovarian cancer. Best Pract Res Clin Obstet Gynaecol, 2017; 41: 3-14. DOI: 10.1016/j.bpobgyn.2016.08.006
[3] Lheureux S, Gourley C, Vergote I et al. Epithelial ovarian cancer. Lancet, 2019; 393: 1240-1253. DOI: 10.1016/S0140-6736(18)32552-2
[4] Euscher ED. Germ cell tumors of the female genital tract. Surg Pathol Clin, 2019; 12: 621-649. DOI: 10.1016/j.path.2019.01.005
[5] Hanley KZ, Mosunjac MB. Practical review of ovarian sex cord-stromal tumors. Surg Pathol Clin, 2019; 12: 587-620. DOI: 10.1016/j.path.2019.02.005
[6] Teeuwssen M, Fodde R. Wnt signaling in ovarian cancer stemness, EMT, and therapy resistance. J Clin Med, 2019; 8: 1658. DOI: 10.3390/jcm8101658
[7] Lheureux S, Braunstein M, Oza AM. Epithelial ovarian cancer: Evolution of management in the era of precision medicine. CA Cancer J Clin, 2019; 69: 280-304. DOI: 10.3322/caac.21559
[8] Lu Z, Chen J. Introduction of WHO classification of tumours of female reproductive organs, fourth edition. Chinese J Pathol, 2014; 43: 649-650.
[9] Piche A. Malignant peritoneal effusion acting as a tumor environment in ovarian cancer progression: Impact and significance. World J Clin Oncol, 2018; 9: 167-171. DOI: 10.5306/wjco.v9.i8.167
[10] Takahara N, Isayama H, Nakai Y et al. Pancreatic cancer with malignant ascites: clinical features and outcomes. Pancreas, 2015; 44: 380-385. DOI: 10.1097/MPA.0000000000000290
[11] Raymond SLT, Au K, Fu R et al. Metastatic genitourinary cancer diagnosed by body fluid cytology: clinicopathologic and cytomorphologic correlation. J Am Soc Cytopathol, 2017; 6: 48-58. DOI: 10.1016/j.jasc.2016.11.001
[12] Donnenberg AD, Luketich JD, Dhupar R et al. Treatment of malignant pleural effusions: the case for localized immunotherapy. J Immunother Cancer, 2019; 7: 1-5. DOI: 10.1186/s40425-019-0590-4
[13] Gu F, Wu J, Liu Y et al. Human inflammatory dendritic cells in malignant pleural effusions induce Th1 cell differentiation. Cancer Immunol Immun, 2020; 69: 779-788. DOI: 10.1007/s00262-020-02510-1
[14] Heinrich S, Lang H. Neoadjuvant Therapy of Pancreatic Cancer: Definitions and Benefits. Int J Mol Sci, 2017; 18: 1622. DOI: 10.3390/ijms18081622
[15] Kumar V. Natural killer cells in sepsis: Underprivileged innate immune cells. Eur J Cell Biol, 2019; 98: 81-93. DOI: 10.1016/j.ejcb.2018.12.003
[16] Lister J, Rybka WB, Donnenberg AD et al. Autologous peripheral blood stem cell transplantation and adoptive immunotherapy with activated natural killer cells in the immediate posttransplant period. Clin Cancer Res, 1995; 1: 607-614.
[17] Tejera B, Lopez RE, Hidalgo P et al. The human adenovirus type 5 E1B 55kDa protein interacts with RNA promoting timely DNA replication and viral late mRNA metabolism. PLoS One, 2019; 14: e0214882. DOI: 10.1371/journal.pone.0214882
[18] Hammer Q, Ruckert T, Romagnani C. Natural killer cell specificity for viral infections. Nat Immunol, 2018; 19: 800-808. DOI: 10.1038/s41590-018-0163-6
[19] Bahr I, Jahn J, Zipprich A et al. Impaired natural killer cell subset phenotypes in human obesity. Immunol Res, 2018; 66: 234-244. DOI: 10.1007/s12026-018-8989-4
[20] Chen T, Liu C, Li L et al. CD56bright natural killer cells exhibit abnormal phenotype and function in severe aplastic anemia. Int J Lab Hematol, 2019; 41: 353-363. DOI: 10.1111/ijlh.12982
[21] Mukherjee N, Ji N, Hurez V et al. Intratumoral CD56 (bright) natural killer cells are associated with improved survival in bladder cancer. Oncotarget, 2018; 9: 36492-36502. DOI: 10.18632/oncotarget.26362
[22] He CB, Lin XJ. Inflammation scores predict the survival of patients with hepatocellular carcinoma who were treated with transarterial chemoembolization and recombinant human type-5 adenovirus H101. PLoS One, 2017; 12: e0174769. DOI: 10.1371/journal.pone.0174769
[23] Campos-Da-Paz M, Dorea JG, Galdino AS et al. Carcinoembryonic antigen (CEA) and hepatic metastasis in colorectal cancer: Update on biomarker for clinical and biotechnological approaches. Recent Pat Biotechnol, 2018; 12: 269-279. DOI: 10.2174/1872208312666180731104244
[24] Bian J, Li B, Kou XJ et al. Clinical applicability of multi-tumor marker protein chips for diagnosing ovarian cancer. Asian Pac J Cancer P, 2014; 15: 8409-8411. DOI: 10.7314/apjcp.2014.15.19.8409
[25] Zhang W, Wang L, Xin Z. Combination of serum CA19-9 and CA125 levels and contrast-enhanced ultrasound parametric data facilitates to differentiate ovarian serous carcinoma from ovarian malignant epithelial cancer. Medicine (Baltimore), 2018; 97: e0358. DOI: 10.1097/MD.0000000000010358
[26] Sauzay C, Petit A, Bourgeois AM et al. Alpha-foetoprotein (AFP): A multi-purpose marker in hepatocellular carcinoma. Clin Chim Acta, 2016; 463: 39-44. DOI: 10.1016/j.cca.2016.10.006
[27] Isgro MA, Bottoni P, Scatena R. Neuron-specific enolase as a biomarker: biochemical and clinical aspects. Adv Exp Med Biol, 2015; 867: 125-143. DOI: 10.1007/978-94-017-7215-0_9
[28] Andre P, Denis C, Soulas C et al. Anti-NKG2A mAb is a checkpoint inhibitor that promotes anti-tumor immunity by unleashing both T and NK cells. Cell, 2018; 175: 1731-1743.e1713. DOI: 10.1016/j.cell.2018.10.014
Copyright © 2021 The Author(s). This open-access article is licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, sharing, adaptation, distribution, and reproduction in any medium, provided the original work is properly cited.


