Quantitative Impacts of Normalizing Gluttony: Case Study of the USA
Joshua M. Pearce1,2*
1School of Ivey Business, Western University, London, Canada
2Department of Electrical & Computer Engineering, Western University, London, Canada
*Correspondence to: Joshua M. Pearce, PhD, Professor, Department of Electrical & Computer Engineering, Western University, London, ON, N6A 5B9, Canada; Email: joshua.pearce@uwo.ca
DOI: 10.53964/jia.2024011
Abstract
Various cultures throughout history may have established social norms around the concept of sins for pragmatic community health reasons. The concept of sin, however, has largely disappeared with the rise of modern cancel culture. Now secular society routinely normalizes all sins including the historical 'seven deadly sins', which provides a natural experiment to determine the consequences of normalizing the concept of sin. In this study, gluttony, which is defined here as the overindulgence in food, is analyzed. First, substantial evidence is provided that gluttony was first ignored and then normalized in modern U.S. society with the body positive and fat acceptance movements becoming mainstream. Then, the health and economic impacts of the expanded gluttony are quantified for the society of those practicing gluttony. The results show ignoring the concept of gluttony as a sin has correlated with a steady increase in the rate of obesity in America. Now 73.6% of the American public is overweight and obese. The U.S. now has more obese people than normal weight or overweight people. This has severe negative impacts on the health of individuals that are overweight as well as the community as a whole. Altogether the overweight and obese are expected to lose an aggregate of > 100 million life years while suffering from a wide range of concomitant diseases. In addition, the obese increase medical costs for Americans by $173 billion and the expected impacts of childhood obesity will add up to another $49 billion by midcentury. It can be safely concluded that normalizing the concept of the sin of gluttony in the U.S. has an aggregate negative impact on U.S. society.
Keywords: gluttony, health policy, sin, obesity, overweight
1. INTRODUCTION
Historically, the concept of sin is Christianity has been characterized as actions in conflict with the behaviors and patterns of life to which God wants humanity to follow[1]. The specific "seven deadly sins"[2], which is a classification of the worst vices within Christian thought include: pride, greed, wrath, envy, lust, gluttony and sloth[3]. In general, most Americans were Christian (as recently as the early 1990s, about 90% of U.S. adults identified as Christians )[4]. and thus, historically most Americans would thus be expected to attempt to avoid what they would consider vices (or sins) as much as they were able on religious grounds. As Christianity has declined in the U.S.[5], however, so too has the concept of sin fallen out of favor in the general public discourse[6]. More than twenty years ago, Plantinga has documented, "the shadow of sin has now dimmed" in public consciousness to the point that "Even preachers…. now speak of sin in a mumble"[7]. All cultures had a sense of right and wrong[8] and the classification of sins may have developed around pragmatic and useful reasons[9].This then would be similar to the philosophical arguments for the pragmatic beliefs in theism[10-12]. Thus, as secular U.S. culture has pushed to "cancel" the concept of sin as expressions of personal choice, are there repercussions for dismissing vices?
To explore this question quantitively, this study reviews the concept of sin applied to gluttony, which is defined here as the over-indulgence and over-consumption of food. Often over-consumption of drink is included as well, but is left for future work. First, evidence that modern U.S. culture has normalized gluttony will be reviewed. Then, the health, social and economic impacts of expanded gluttony will be quantified to the best degree possible while outlining weaknesses, missing data, and necessary assumptions. Finally, all of these impacts of the modern embrace of gluttony will be summarized in the context of public health.
2. NORMALIZATION OF GLUTTONY IN THE U.S.
Historically, gluttony had been roundly condemned[13]. Through the eighteenth century, however, "gluttony lost some of its stigma and eventually became almost a badge of pride"[14]. Today there are several signs that gluttony has been 'normalized' as a form of 'self care'.
First, food has become more abundant and convenient to acquire and consume in the U.S. thereby making gluttony easier. Historically, there was something of a limit to overindulgence and the concomitant fat a human could accumulate, which was simply restricted by the availability and difficulty of acquiring food. For example, American Indian populations only developed obesity in the past 1-2 generations, with the historically-unprecedented relative abundance of high-fat foods that could be acquired even with those living a similarly historically-unprecedented sedentary lifestyle[15]. Today 48.1% of native Americans are obese[16]. The ready availability of low-cost calories that may not be nutritious is apparent throughout the U.S. and exacerbated in isolated communities[17]. Overall most Americans consume poor diets[18] and the rate of overweight and obese Americans has risen dramatically[19]. Refined grains, added sugars, and added fats are among the lowest-cost sources of dietary energy and remarkably convenient[20].
The convenience of the modern U.S. food system can hardly be overstated. Not only is there readily available prepared food at restaurants, but also in gas stations, specialty shops and even in vending machines. Over 40% of food expenditures are outside of the home[21], where large portion sizes and added fat are the norm. This is readily observed by the positive association between frequency of consuming restaurant food with body fatness[22]. American food consumers, however, no longer even need to leave home due to conventional food delivery (e.g., the ubiquity of delivery pizza or American 'Chinese food'). Now, however, there is also a plethora of companies competing with low-paid 'gig economy' workers[23,24] to deliver any type of food to a person's home including: ChowNow, DoorDash, Grubhub, Deliveroo, Deliverect, Just Eat, Skip The Dishes, Chat Food, Instacart, Uber Eats, and many more. Similarly, there is also widespread use of delivery groceries from conventional grocery stores as well as Wal-Mart and internet stores like Amazon, which became widespread during the COVID-19 pandemic[25]. Finally, adults now consume more than 57% of their calories from ultra-processed foods[26] and children do at 67%[27]. All of this ensures that the extremely obese can continue to acquire calories without having to leave their homes. Consider for example, that firefighters have been used to extract people that have become so obese they are unable to move out of their residences through doors[28]. It should also be noted that this obesity-generating food system focused on ultra processed foods is highly unsustainable[29,30] and thus also has secondary impacts on human health after obesity. For example, ultra processed foods are responsible for 36–45% of total diet-related biodiversity loss and a third of diet-related greenhouse gas emissions[31], which in turn cause a litany of health issues[32-34] and mortality[35-39].
Second, many American cultural practices encourage overconsumption of food and thus gluttony even from an early age. Many people live in what is described as healthy food deserts, where the food options are all unhealthy highly processed foods[40]. Simultaneously, convenience stores and fast food restaurants, which sell low-cost unhealthy food, are abundant and purposefully located close to schools to profit from target marketing youth[41,42]. Even schools that offer a la carte options provide harmful training in poor food selections using pricing strategies, which results in children choosing larger bags of high-fat, high-salt snacks inside the schools[43]. A similar cultural practice for adults is seen in increasing portion sizes for processed foods. This is also known to be an environmental contributor to obesity[44]. For example, it is well established that food vendors can extract large profits by using "supersizing" strategies where regular portion sizes are priced high enough to discourage price-conscious consumers from selecting them, and instead the prices for enlarging food portions are set low enough that these customers order the larger portion sizes and overeat[45]. In the U.S. large portion sizes of highly palatable food that lead to overeating[46] have become the norm both at restaurants as well as at home. The ease of gluttony, where consumers overeat even with a single food item, has increased with time in restaurants as seen in Figure 1[47]. Burger King's Whopper was released in 1957 and for decades remained virtually unchanged. Then the Double Whopper was introduced in 1996 taking the calories per sandwich up 240 calories and the Triple Whopper was introduced in 2005 roughly doubling the calories of the initial Whopper[48]. Today the Roadhouse King has more than double the calories than in the initial sandwich. The trend appears to be obvious, and sandwiches will continue to grow. It should be noted that the Roadhouse King already challenges the jaw opening maximum of many humans, it might be predicted the next sandwich will be longer (e.g., like their Long Burger, but perhaps triple stacked). For context a single Whopper alone (no fries, drink or dessert) would be roughly the calories for one meal (of three a day) for a person on a 2000 calorie per day diet. Eating any of the modern Whoppers with normal sides push adults over their recommended daily allowance of calories.
Similar issues of insidious gluttony also occur for those that eat at home. For example, a cross-cultural study observed that recipe portions of the same dishes from popular cookbooks were 25% larger in the U.S. than in France[49]. It should be noted that the U.S. is not alone in suffering from social trends that encourage obesity. For example, a study in Australia noted that experts identified the most important social trends contributing to obesity as 'escalating car reliance', 'lack of time/increasing business' and 'rising use of convenience and pre-prepared food'[50].
|
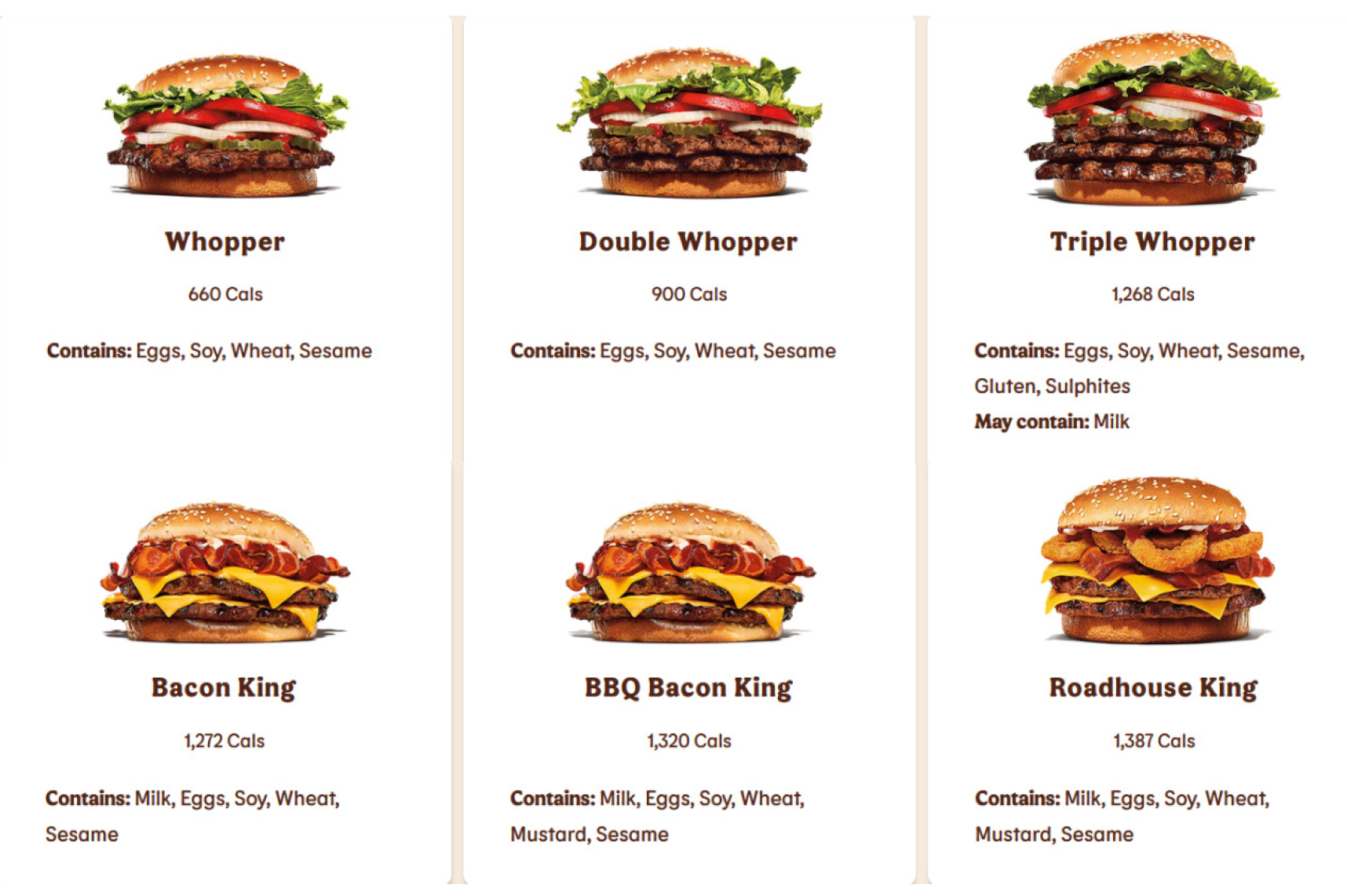
Figure 1. Calories in single sandwiches at Burger King.
Similarly, the proliferation of all-you-can-eat restaurants has made overeating much easier than at conventional restaurants where there is a cycle of order/prepare/eat that sets time limits on the number of calories an individual can consume during a meal. For example, buffet chains such as Golden Corral and Sizzler offer unlimited food at a flat rate and even Red Lobster tried (and failed because of the extreme gluttony of their customers[51]) to recover from the pandemic with $20 for unlimited shrimp[52]. Many all you can eat buffet restaurants, however, quickly rebounded after the pandemic[53]. Former employees of Olive Garden (a restaurant that provides limitless food) reported that adults often throw up to eat more[54]. This is the literal definition of gluttony.
Gluttony has gained so much popularity it has even become a 'sport' including exhibition eating[55] and competitive eating[56]. This new sport of gluttony has become so mainstream that it has formed its own league: Major League Eating (MLE), which is a body that oversees all professional eating contests. To understand how widespread gluttony is celebrated in the U.S. consider MLE description of their impact on American society[57]:
“MLE promotions generate billions of consumer impressions annually. The Nathan's Famous contest generated more than 300 million consumer impressions on domestic television and hundreds of million more impressions in traditional and digital media. Outlets that have covered our events in the past year include ESPN, CNN, FOX, BBC, Yahoo.com, Vice.com, Reuters, NBC News, ABC News, FOX News, CBS News, the Today Show, Good Morning America, the Tonight Show, The Late Show, the Jimmy Kimmel Show, Associated Press, Sports Illustrated, the New York Times, the Wall Street Journal, and thousands of network television affiliates, newspapers, and radio stations nationwide.”
In this context of abundant, low-cost, convenient high calorie food as well as cultural practices that celebrate gluttony and a preponderance of large businesses profit from it, activists have pushed to normalize being overweight and obese. The body positive movement, for example, has flourished in the U.S. In the article "What Is Body Positivity?: The Path from Shame to Pride" body positivity is defined as a movement to accept bodies, regardless of size and shape, as well as other factors[58]. (It should be noted that pride is also one of the deadly sins and an analysis of celebrating the sin of pride is left for future work.) Body positivity aims to challenge dominant appearance ideals[59] and is supported by some academics[60]. It is predominantly done on the social media platform of Instagram, where people are encouraged to post pictures of themselves with the hashtag #bodypositivity and supportive messages related to a positive self-image[61]. As the body positive movement became normalized in American society, some authors have claimed it has become commodified as companies launched plus size clothing lines and included plus sized models in advertising campaigns[62]. Critics of the body positive movement, point out that it simply was changing society's expectations of obesity, rather than changing the individual behaviors that contribute to obesity and negative health outcomes[63]. There is some evidence that one result of the body positive movement and normalizing plus sizes is people's inability to accurately gauge how overweight or obese they are, which makes them 85% less likely to try to lose weight compared with people who accurately identified their weight status[64]. Thus, normalizing obesity using various social influencing mechanisms[65] can explain in part the prevalence of obesity.
Taking the next step in the normalization of obesity is the 'fat acceptance movement' or 'fat activism' (also referred to as fat pride, fat empowerment, and fat liberation), which is a social movement that seeks to eliminate the social stigma of obesity entirely[66]. These activists are supported by academics who argue against fat stigma as well as strategies to diminish focus on personal responsibility (e.g., sin)[67]. As the fat acceptance movement argues against the predominant view that being obese is unhealthy, critics thus question if the fat acceptance movement is bad for health[68]. Being fat in the U.S. is now 'in', however, and readily accepted[69]. At this point it appears that even extreme morbid obesity has lost most of the stigma and that has occurred over forty years of fat activism, which has been supported by elements of feminism, queer theory and anti-racism[70].
3 RESULTS
As the preceding section has shown, gluttony has become normalized in the U.S. The following section will attempt to quantify the impacts of that normalization in health and economic impacts.
With gluttony becoming accepted in the U.S. overeating has become common and this has resulted in a historically unprecedented number of overweight people in the population using measured heights and weights. According to 2017–2018 data from the National Health and Nutrition Examination Survey (NHANES) 42.5% of U.S. adults aged 20 and over have obesity, including 9.2% with severe obesity, and another 31.1% are overweight[71]. Thus, roughly only a quarter of the U.S. population is a healthy weight for their height. The historical trends are shown in Figure 2. Prior to 1960 severe obesity was extremely uncommon and now for women, who are more likely to ascribe to the body positive movement, it is approaching 1 in 10. Obesity for both men and women has climbed by more than a factor of four. At first inspection of the line for overweight men it appeared that it has been constant and even declined recently. A likely explanation of this trend put in context is that overweight men are becoming obese and formally healthy weight men are becoming more likely to be overweight.
|
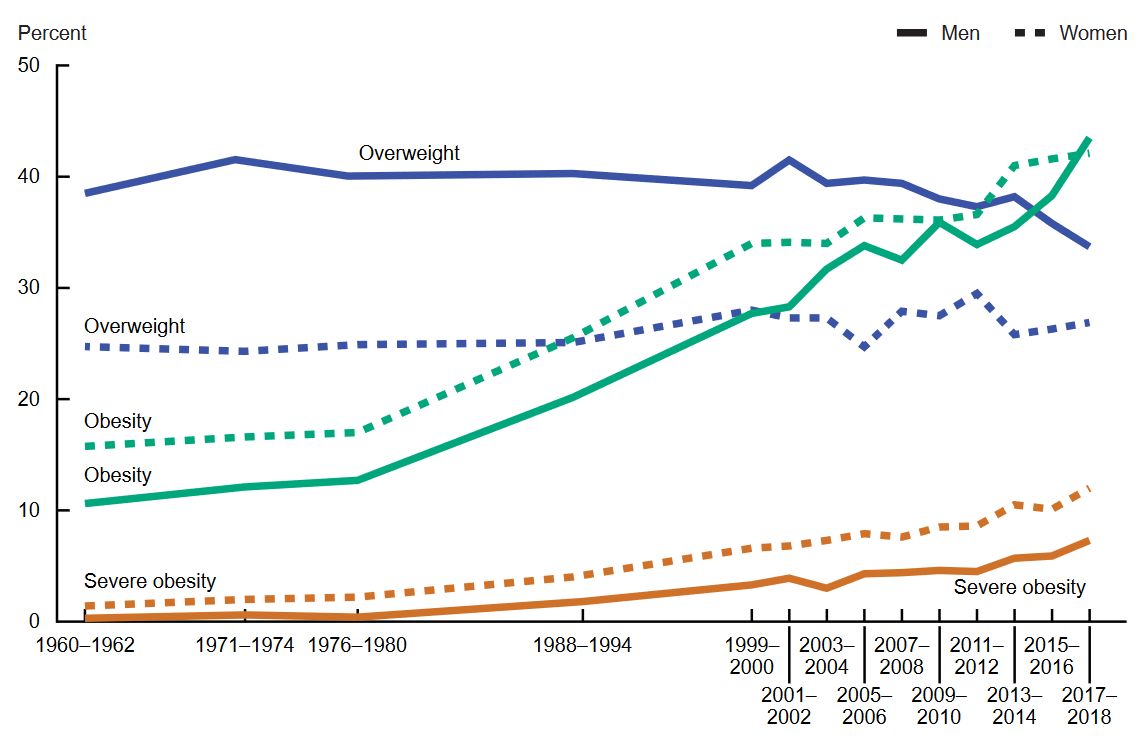
Figure 2. American adults 20-74 years old that are overweight, obese, and or have severe obesity among men and women.
Gluttony is also impacting America's youth as the NHANES results show 19.3% of U.S. children and adolescents aged 2–19 years have obesity, including 6.1% with severe obesity, and another 16.1% are overweight[72]. Thus, over 35% of children now suffer from the heath impacts of gluttony. These values are lower than those for adults because children still tend to be more active, and they have not had enough time to increase their weight. This is seen in Figure 3, that younger children suffer from obesity to a smaller degree than older children[72]. It is also clear that obesity in children has increased by factors of 3 to 4 since the 1960s.
|
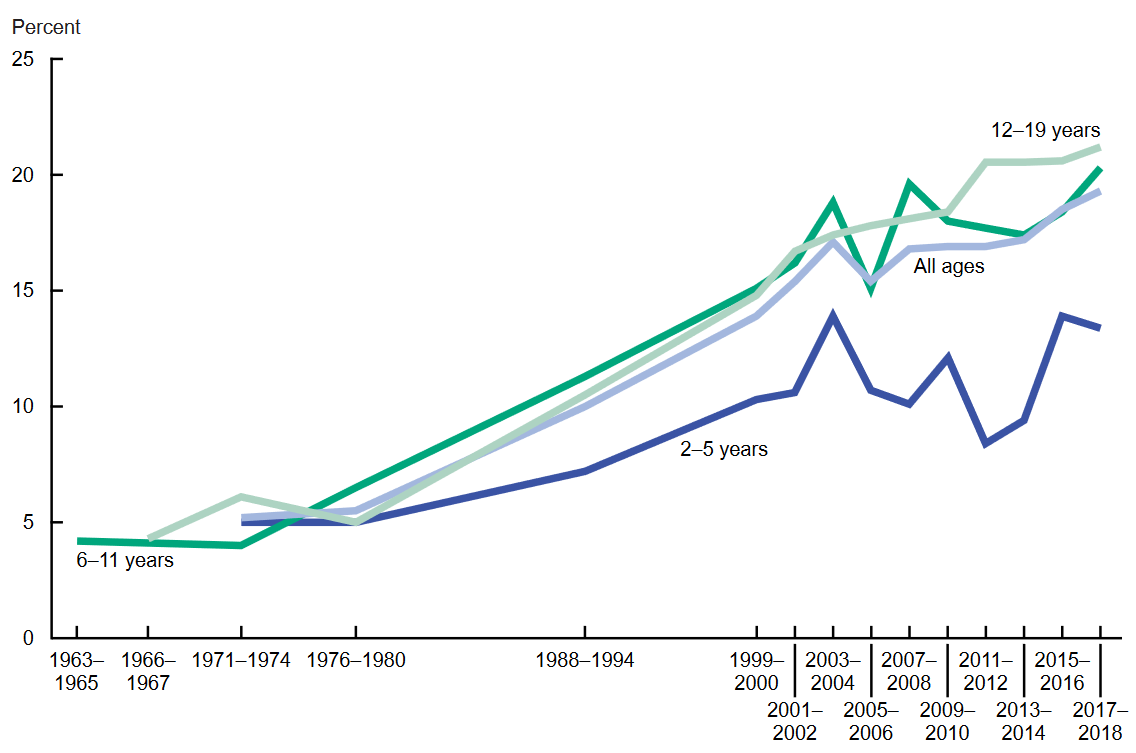
Figure 3. Historical obesity among American children and adolescents aged 2-19 years, by age.
Counter to claims made by the fat acceptance movement, obesity has severe negative impacts on human health and is widely regarded as a public health hazard. It is well established in the medical community that obesity is a significant risk factor for and contributor to increased morbidity and mortality. Life expectancy of obese people is reduced following models in the literature that tie obesity to other diseases. This is because obesity strongly contributes to deaths from cardiovascular disease and type 2 diabetes[73], but also from hyperlipidemia, hypertension, stroke, cancer (e.g., breast and colon cancer) and chronic diseases such as osteoarthritis, liver and kidney disease, sleep apnea, and even depression[74,75]. Obesity is also strongly associated with an increased risk mortality as well as specific cardiovascular and cancer mortality[74]. Obesity may have a significant impact on quality-adjusted life years, with extreme obesity expected to shorten lifespan by 14 years[76]. In 2012 the aggregate years-of-life-lost from obesity was estimated at ∼95 million[77] and given the rapid rise in obesity since then shown in Figure 2 the number is conservatively above 100 million as of this writing. With the life expectancy in the U.S. about 78 years this is equivalent to sacrificing more than 1.2 million people's entire lives for obesity. Despite the substantial negative effects of obesity, weight loss from reducing the ratio of calories expended to calories consumed can result in a significant reduction in risk for the majority of these comorbid conditions.
The adverse medical impacts of gluttony in the U.S. have direct economic costs for both adults and children[78]. Each obese adult can expect to have an extra $1,861 (95% CI $1,656-$2,053) medical costs per year[79]. This can be a substantial burden on low-income individuals. For example, with the federal minimum wage being $7.25/hour[80] a minimum wage worker would need to work 256 hours (or 6.4 full time weeks) to cover the 'obesity tax'. Severe obesity, as expected is even worse with excess costs of $3,097 (95% CI $2,777-$3,413) per year per adult[79], which is equivalent to 427 hours of work (10.6 weeks or about 2.5 months of full time work) at the minimum wage. Obese children have an extra $116 (95% CI $14-$201) which is $1.32 billion (95% CI $0.16-$2.29) of medical spending, with severe obesity associated with $310 (95% CI $124-$474) excess costs per child[79]. These examples assume those with obesity were employed, although in reality obese people are less likely to be employed and they are more likely to be absent from work because of sickness (particularly for those with severe obesity who are more likely to call in sick)[81]. It should also be pointed out that a substantial part of the lower wages among obese often attributed to labor market discrimination can actually be explained by their higher health insurance premiums[82]. In addition, childhood obesity causes increases in health care costs in nonhospital healthcare, outpatient visits, medication, and hospitalization that follow obese individuals as they grow up (annual direct and indirect costs were projected to be $13.62 billion and $49.02 billion by 2050 from this alone)[83]. Overall a significant percent of overall healthcare costs in the U.S. are a direct result of Americans being overweight and obese[78] and altogether, obesity increases medical costs for Americans by $172.74 billion (95% CI $153.70-$190.61)[79].
4 DISCUSSION
Despite, the obvious negative consequences to both health and economic wellbeing, some argue, that fat shaming or weight discrimination is more important and is now comparable to prevalence rates of racial discrimination in America[84]. This is difficult to understand if such large numbers of Americans are overweight and obese, easily making up a large majority. In addition, some authors have stressed the enormous growth and overall success of the body positive movement and fat acceptance movement[85], which would not be the case if the discrimination was the main problem. Others have argued for an 'obesity paradox' and 'healthy obese', however, medical/scientific studies have clearly shown obese individuals, regardless of their metabolic status (healthy or unhealthy) are at increased risk for adverse health outcomes from being obese, when compared to individuals with a normal weight[86]. Thus there is no healthy obese status.
Other critics may point out that as obesity rates have climbed many scientific studies have found other causes of obesity. Although obesity is most commonly caused by an excess energy consumption from eating relative to energy expenditure from metabolic and physical activity, the causes of obesity are highly complex and include genetic, physiologic, environmental, psychological, social, economic, and even political factors[87]. These different causes interact in various ways and by varying degrees to promote the development of obesity other than simply overeating. Critics may point out that individuals being obese and overweight may not be from gluttony as these conditions have several reasons, including genetic, metabolic, behavioral and environmental causes, however, the recent rapid increases in the prevalence suggests that this is indeed due to behavioral and environmental influences, rather than biological changes[88]. It is certainly true that studies have shown losing fat mass can have adverse effects on appetite control and even reduce energy expenditures, increasing the challenge of losing more weight[89] thus weight change can become self-limiting[90]. Without overeating, however, the initial energy ration of input over output could not have caused the weight gain.
Rosen has argued that in our society, labeling obesity as a disease was necessary to improve attitudes, increase resources for health promotion and research into causes (behavioral, environmental, and genetic) and financial support for obesity prevention and treatment (medical and surgical)[91]. Obesity has been considered a disease for more than a decade and as Figures 2 and 3 show, society has made no progress while the media leans hard into the idea that it is genetic[92,93]. Although the idea that obesity is genetic is obviously appealing to three quarters of the American public that is overweight or obese, the historical record indicates it has far more to do with other factors including the self-control of the individual in an unquestionably obese-inducing environment of modern America.
The results of this study bring up some interesting possibilities and many questions. First, correlation of obesity and poor health outcomes with the decline of the concept of sin does not necessarily indicate that it is causal. Thus, the question remains, if ignoring the concept of sin and normalizing gluttony while considering the obesity result as a disease has been utterly ineffective at even reducing the negative health impacts as well as the rate of obesity, what would the impact be of stressing that gluttony is a sin? There is already some evidence that religious leaders' messages against excessive eating is associated with a significantly lower probability of being overweight or obese[94]. Similarly attending religious services was something of a shield against excessive weight gain recently observed during the COVID-19 pandemic[95]. Substantial future work is needed in this area of empirical studies that show evidence of the impacts of religion on obesity as the few studies to date are extremely promising. Would individuals eat less, be more careful about what foods they put in their bodies and exercise more if they strongly considered gluttony as a sin? Would it discourage overeating in the public and decrease sales of the higher caloric foods such as shown in Figure 1? If consideration of gluttony as a sin was widespread, would company leaders voluntarily manipulate the market to encourage healthy food and smaller servicing sizes instead of supersizing everything? Would politicians help their constituents reduce gluttony by for example switching subsidies to low-processed fruits and vegetables? Clearly substantial future work is warranted in this area as the concept of sin may be extremely beneficial to community health. There are counter examples (e.g., in some communities illness is viewed as a punishment for sin[96] and can be used as a reason not to seek medical treatment). In addition future work could compare the effectiveness of the concept of sin to reverse obesity compared to other health measures such as more traditional legislation, regulation, and health policy to address the multiple factors that contribute to obesogenic environments[97].
Similarly improving the distribution of the concept of sin, which would be considered an 'upstream' policy intervention could be compared to others (e.g. taxation, education, social security) or encouraging supportive environments with healthy food and physical activity or 'midstream' to influence behavior or 'downstream' policies that support health/clinical interventions[98]. It would also be interesting to perform an economic analysis on the costs and benefits of encouraging the proliferation of the concept of sin against other policy methods such as sugar taxes[99] or subsidies for healthy food choices[100,101]. Substantial future work is needed, however, to determine mechanisms and costs for expanding the concept of sin in the general public. In addition, any potential recommendation to reinvigorate the concept of sin as a public health tool raises ethical concerns. How can this be done while maintaining a pluralistic society with diverse moral and multiple religions? For example, a straight-forward approach might be enabling religious-focused public schools as has been done in Canada for Catholic schools. In Canada, the Catholic schools generally have advantages for academic performance over the secular schools[102], which would be an additional benefit to the potential health gains because of the greater distribution of the concept of sin. This would need to be analyzed carefully as for example Catholic schools in Canada have many (and in some cases the majority) of non-practicing Catholics and students of other or no religion attending them. There is, of course, no guarantee this would always be the case, nor the impact on society if all of the educational system was balkanized into different religions be a net positive. Substantial future work is needed to consider the overall impacts of state-supported religious education, even for the potential advantages to health and human quality of life.
This study has several limitations. First, this study did not attempt to quantify the secondary benefits of society embracing gluttony. For example, although gluttony leads to obesity and poor health outcomes, these poor health outcomes create health care industry revenue and increase employment by offering more health-care-related jobs. Similarly, as adults become more obese they would need larger clothes, chairs, etc., which could increase retails sales of plus-size clothing, larger chairs that can handle more mass, as well as other products sold by body positive companies that profit from obesity[103]. Also overweight and obese people die prematurely, which Allison et al., have pointed out that the increased costs of healthcare for obese people is somewhat tempered by their greater mortality rates[104]. It can be assumed, however, that most people would not consider increased disease to drive up medical industry revenue or products sales a net benefit, nor would they count dying to conserve some end of life medical costs as a net benefit.
5 CONCLUSIONS
This study has shown that as the concept of gluttony as sin was first ignored and then normalized in modern U.S. society the body positive and fat acceptance movements were able to claim success. These movements are supported by companies that profit from selling products that encourage overindulgence of food. The results of ignoring the concept of sin of gluttony, however, have been profound with a steady increase in the rate of obesity in America. Now more than 73.6% of the American public is overweight and obese. The U.S. now has more obese people than normal weight or even overweight people. This has severe negative impacts on human health of individuals that suffer from it. The 9.2% of Americans with extreme obesity are expected to shorten their lives by 14 years. Altogether the overweight and obese are expected to lose an aggregate of more than 100 million life years while suffering from a wide range of diseases. Obesity also has a major negative impact on the finances of those that suffer the consequences of gluttony. Today obesity increases medical costs for Americans by $172.74 billion and the impacts of childhood obesity are projected to add another $13 to $49 billion by midcentury. It can be safely concluded that normalizing the sin of gluttony in the U.S. has an aggregate negative impact on U.S. society. Future work is needed to determine how a resurgence of the concept of sin in general and gluttony in particular may improve health and economic outcomes for those that currently suffer from the consequences of gluttony.
Acknowledgements
This work was supported by the Thompson Endowment.
Conflicts of Interest
The author declared no conflict of interest.
Author Contribution
The author wrote the manuscript and approved the final version.
Abbreviation List
CI: Confidence interval
MLE : Major League Eating
NHANES: National Health and Nutrition Examination Survey
References
[1] Timpe K. Sin in Christian Thought. Accessed 19 March 2024. Available at:[Web]
[2] Lyman SM. The Seven Deadly Sins: Society and Evil. Rowman & Littlefield: Maryland, USA, 1989.
[3] Tucker SR. The Virtues and Vices in the Arts : A Sourcebook. Accessed 19 March 2024. Available at:[Web]
[4] Nadeem R. How U.S. religious composition has changed in recent decades. Accessed 23 July 2024. Available at:[Web]
[5] Center PR. In U.S., Decline of Christianity Continues at Rapid Pace. Accessed 19 March 2024. Available at:[Web]
[6] Yoffie E. Why Americans Dismiss Sin. Accessed 19 March 2024. Available at:[Web]
[7] Plantinga C. Not the Way It's Supposed to Be: A Breviary of Sin. Wm. B. Eerdmans Publishing: Grand Rapids, USA, 1996.
[8] Dye TW. Toward a Cross-Cultural Definition of Sin. Missiology, 1976; 4: 27-41.[DOI]
[9] Salomon DA. The Seven Deadly Sins: How Sin Influenced the West from the Middle Ages to the Modern Era. Bloomsbury Publishing USA: New York, USA, 2019.
[10] Jordan J. Pragmatic Arguments and Belief in God. 2004. Accessed 19 March 2024. Available at:[Web]
[11] JORDAN J. Pascal's Wager: Pragmatic Arguments and Belief in God. Clarendon Press: Oxford, England, 2006.
[12] Jackson E. Pragmatic Arguments for Theism. The Cambridge Handbook of Religious Epistemology. Cambridge University Press: Cambridge, UK, 2023.
[13] Hill SE. Eating to Excess: The Meaning of Gluttony and the Fat Body in the Ancient World. Bloomsbury Publishing USA: New York, USA, 2011.
[14] Prose F. Gluttony : The Seven Deadly Sins: The Seven Deadly Sins. Oxford University Press: New York, USA, 2003.
[15] Welty T. Health Implications of obesity in American Indians and Alaska Natives. Am J Clin Nutr, 1991; 53: 1616S-1620S.[DOI]
[16] HHS. Obesity and American Indians/Alaska Natives | Office of Minority Health. Accessed 12 April 2024. Available at:[Web]
[17] Kenny TA, Fillion M, MacLean J et al.. Calories are cheap, nutrients are expensive – The challenge of healthy living in Arctic communities. Food Policy, 2018; 80: 39-54.[DOI]
[18] Carlson A, Frazão E. Food costs, diet quality and energy balance in the United States. Physiol Behav, 2014; 134: 20-31.[DOI]
[19] Phelan S. Obesity in the American population: calories, cost, and culture. Am J Obstet Gynecol, 2010; 203: 522-524.[DOI]
[20] Drewnowski A, Darmon N. The economics of obesity: dietary energy density and energy cost. Am J Clin Nutr, 2005; 82: 265S-273S.[DOI]
[21] Paulin GD. Let's Do Lunch: Expenditures on Meals Away from Home Spending Patterns. Mon Labor Rev, 2000; 123: 36-45.
[22] McCrory MA, Fuss PJ, Hays NP et al. Overeating in America: Association between Restaurant Food Consumption and Body Fatness in Healthy Adult Men and Women Ages 19 to 80. Obes Res, 1999; 7: 564-571.[DOI]
[23] Friedman G. Workers without employers: shadow corporations and the rise of the gig economy. Rev Keynes Econ, 2014; 2: 171-188.[DOI]
[24] Healy J, Pekarek A. Work and wages in the gig economy: can there be a high road? The Future of Work and Employment. Edward Elgar Publishing: Cheltenham , UK, 2020.
[25] Delasay M, Jain A, Kumar S. Impacts of the COVID-19 pandemic on grocery retail operations: An analytical model. Prod Oper Manag, 2022; 31: 2237-2255.[DOI]
[26] Juul F, Parekh N, Martinez-Steele E et al. Ultra-processed food consumption among US adults from 2001 to 2018. Am J Clin Nutr, 2022; 115: 211-221.[DOI]
[27] Wang L, Steele EM, Du M et al. Trends in Consumption of Ultraprocessed Foods Among US Youths Aged 2-19 Years, 1999-2018. JAMA, 2021; 326: 519-530.[DOI]
[28] CNN. 800-pound man cut from home after fall. Accessed 19 March 2024. Available at:[Web]
[29] Seferidi P, Scrinis G, Huybrechts I et al. The neglected environmental impacts of ultra-processed foods. Lancet Planet Health, 2020; 4: e437-e438.[DOI]
[30] Kesse-Guyot E, Allès B, Brunin J et al. Environmental impacts along the value chain from the consumption of ultra-processed foods. Nat Sustain, 2023; 6: 192-202.[DOI]
[31] Anastasiou K, Baker P, Hadjikakou M et al. A conceptual framework for understanding the environmental impacts of ultra-processed foods and implications for sustainable food systems. J Clean Prod, 2022; 368: 133155.[DOI]
[32] Martens P, Mcmichael AJ. Environmental Change, Climate and Health: Issues and Research Methods. Cambridge University Press: Cambridge, UK, 2009.
[33] Haines A, Patz JA. Health Effects of Climate Change. JAMA, 2004; 291: 99-103.[DOI]
[34] Bowles DC, Butler CD, Morisetti N. Climate change, conflict and health. J Roy Soc Med, 2015; 108: 390-395.[DOI]
[35] Parncutt R. The Human Cost of Anthropogenic Global Warming: Semi-Quantitative Prediction and the 1,000-Tonne Rule. Front Psychol, 2019; 10: 2323.[DOI]
[36] Ebi KL, Hess JJ. Health Risks Due To Climate Change: Inequity In Causes And Consequences. Health Affair, 2020; 39: 2056-2062.[DOI]
[37] Vicedo-Cabrera AM, Scovronick N, Sera F et al. The burden of heat-related mortality attributable to recent human-induced climate change. Nat Clim Change, 2021; 11: 492-500.[DOI]
[38] Khraishah H, Alahmad B, Ostergard Jr RL et al. Climate change and cardiovascular disease: implications for global health. Nat Rev Cardiol, 2022; 19: 798-812.[DOI]
[39] Pearce JM, Parncutt R. Quantifying Global Greenhouse Gas Emissions in Human Deaths to Guide Energy Policy. Energies, 2023; 16: 6074.[DOI]
[40] Dubowitz T, Zenk SN, Ghosh-Dastidar B et al. Healthy food access for urban food desert residents: examination of the food environment, food purchasing practices, diet and BMI. Public Health Nutr, 2015; 18: 2220-2230.[DOI]
[41] Austin SB, Melly SJ, Sanchez BN et al. Clustering of fast-food restaurants around schools: a novel application of spatial statistics to the study of food environment. Am J Public Health, 2005; 95: 1575-1581.[DOI]
[42] Kipke MD, Iverson E, Moore D et al. Food and park environments: neighborhood-level risks for childhood obesity in east Los Angeles. J Adolescent Health, 2007; 40: 325-333.[DOI]
[43] Cullen KW, Thompson DI. Texas school food policy changes related to middle school a la carte/snack bar foods: potential savings in kilocalories. J Am Diet Assoc, 2005; 105: 1952-1954.[DOI]
[44] Vermeer WM, Steenhuis IHM, Poelman MP. Small, medium, large or supersize? The development and evaluation of interventions targeted at portion size. Int J Obesity, 2014; 38: S13-S18.[DOI]
[45] Dobson PW, Gerstner E. For a few cents more: Why supersize unhealthy food?. Market Sci, 2010; 29: 770-778.[DOI]
[46] Rolls BJ. The supersizing of America: portion size and the obesity epidemic. Nutr Today, 2003; 38: 42-53.[DOI]
[47] Burger King. Nutrition Explorer - Burger King. Accessed 12 April 2024. Available at:[Web]
[48] Dostal E. The history of Burger King's Whopper. Accessed 12 April 2024. Available at:[Web]
[49] Rozin P, Kabnick K, Pete E et al. The ecology of eating: smaller portion sizes in France than in the United States help explain the French paradox. Psychol Sci, 2003; 14: 450-454.[DOI]
[50] Banwell C, Hinde S, Dixon J et al. Reflections on expert consensus: a case study of the social trends contributing to obesity. Eur J Public Health, 2005; 15: 564-568.[DOI]
[51] Red Lobster Endless Shrimp. Accessed 11 October 2024. Available at:[Web]
[52] X, Instagram, Email. Red Lobster offered customers all-you-can-eat shrimp. That was a mistake. Accessed 11 October 2024. Available at:[Web]
[53] Bondarenko V. In This Economy, The All-You-Can-Eat Buffet Is A Clear Winner. Accessed 19 March 2024. Available at:[Web]
[54] BROGLE C. Former Olive Garden Employee Exposes Horrifying Restaurant Secrets. Accessed 19 March 2024. Available at:[Web]
[55] Wansink B, Kniffin KM. Exhibitionist eating: Who wins eating competitions?. Front Nutr, 2016; 3: 51.[DOI]
[56] Johnson AR. The Art of Competitive Eating. Gastronomy, 2016; 16: 111-114.[DOI]
[57] MLE. About major league eating. Accessed 9 April 2024. Available at:[Web]
[58] Leboeuf C. What is body positivity? The path from shame to pride. Philos Top, 2019; 47: 113-128.[DOI]
[59] Sastre A. Towards a radical body positive: Reading the online “body positive movement”. Fem Media Stud, 2014; 14: 929-943.[DOI]
[60] Cohen R, Newton-John T, Slater A. The case for body positivity on social media: Perspectives on current advances and future directions. J Health Psychol, 2021; 26: 2365-2373.[DOI]
[61] Cohen R, Irwin L, Newton-John T et al. #bodypositivity: A content analysis of body positive accounts on Instagram. Body Image, 2019; 29: 47-57.[DOI]
[62] Cwynar-Horta J. The commodification of the body positive movement on Instagram. Stream, 2016; 8: 36-56.[DOI]
[63] Nomi M. Opinion: Body positivity encourages obesity. Accessed 9 April 2024. Available at:[Web]
[64] Muttarak R. Normalization of plus size and the danger of unseen overweight and obesity in England. Obesity, 2018; 26: 1125-1129.[DOI]
[65] Shoham DA, Hammond R, Rahmandad H et al. Modeling social norms and social influence in obesity. Curr Epidemiol Rep, 2015; 2: 71-79.[DOI]
[66] Puhl RM, Heuer CA. The stigma of obesity: a review and update. Obesity, 2009; 17: 941.[DOI]
[67] Westbury S, Oyebode O, Van Rens T et al. Obesity stigma: causes, consequences, and potential solutions. Curr Obes Rep, 2023; 12: 10-23.[DOI]
[68] Worth T. Is the fat acceptance movement bad for our health? Accessed 9 April 2024. Available at:[Web]
[69] Rabin RC. In the Fatosphere, Big Is In, or at Least Accepted. Accessed 9 April 2024. Available at:[Web]
[70] Cooper C. Fat activism: A radical social movement. Intellect: Bristol, UK, 2021.
[71] Fryar CD. Prevalence of Overweight, Obesity, and Extreme Obesity Among Adults Aged 20 and Over: United States, 1960-1962 Through 2017-2018. Accessed 12 April 2024. Available at:[Web]
[72] Fryar CD. Prevalence of Overweight, Obesity, and Severe Obesity Among Children and Adolescents Aged 2-19 Years: United States, 1963-1965 Through 2017-2018. Accessed 12 April 2024. Available at:[Web]
[73] Finer N. Medical consequences of obesity. Medicine, 2015; 43: 88-93.[DOI]
[74] Pi-Sunyer X. The medical risks of obesity. Postgrad Med, 2009; 121: 21-33.[DOI]
[75] Wells JCK. The evolution of human adiposity and obesity: where did it all go wrong?. Dis Model Mech, 2012; 5: 595-607.[DOI]
[76] Kitahara CM, Flint AJ, Berrington de Gonzalez A et al. Association between class III obesity (BMI of 40-59kg/m2) and mortality: a pooled analysis of 20 prospective studies. PLoS Med, 2014; 11: e1001673.[DOI]
[77] Finkelstein EA, Brown DS, Wrage LA et al. Individual and aggregate years‐of‐life‐lost associated with overweight and obesity. Obesity, 2010; 18: 333-339.[DOI]
[78] Biener A, Cawley J, Meyerhoefer C. The high and rising costs of obesity to the US health care system. J Gen Intern Med, 2017; 32: 6-8.[DOI]
[79] Ward ZJ, Bleich SN, Long MW et al. Association of body mass index with health care expenditures in the United States by age and sex. LoS One, 2021; 16: e0247307.[DOI]
[80] Department of labor. Minimum Wage. Accessed 12 April 2024. Available at:[Web]
[81] Bramming M, Jørgensen MB, Christensen AI et al. BMI and labor market participation: a cohort study of transitions between work, unemployment, and sickness absence. Obesity, 2019; 27: 1703-1710.[DOI]
[82] Bhattacharya J, Bundorf MK. The incidence of the healthcare costs of obesity. J Health Econ, 2009; 28: 649-658.[DOI]
[83] Ling J, Chen S, Zahry NR et al. Economic burden of childhood overweight and obesity: A systematic review and meta‐analysis. Obes Rev, 2023; 24: e13535.[DOI]
[84] Puhl RM, Andreyeva T, Brownell KD. Perceptions of weight discrimination: prevalence and comparison to race and gender discrimination in America. Int J Obesity, 2008; 32: 992-1000.[DOI]
[85] Jennings R. Can social media ever be truly "body positive"?. Accessed 13 April 2024. Available at:[Web]
[86] Kramer CK, Zinman B, Retnakaran R. Are metabolically healthy overweight and obesity benign conditions? A systematic review and meta-analysis. Ann Intern Med, 2013; 159: 758-769.[DOI]
[87] Aronne LJ, Nelinson DS, Lillo JL. Obesity as a disease state: a new paradigm for diagnosis and treatment. Clin cornerstone, 2009; 9: 9-29.[DOI]
[88] Malnick SDH, Knobler H. The medical complications of obesity. J Assoc Phys, 2006; 99: 565-579.[DOI]
[89] Chaput JP, Doucet E, Tremblay A. Obesity: a disease or a biological adaptation? An update. Obes Rev, 2012; 13: 681-691.[DOI]
[90] Katan MB, Ludwig DS. Extra calories cause weight gain—but how much?. JAMA, 2010; 303: 65-66.[DOI]
[91] Rosen H. Is obesity a disease or a behavior abnormality? Did the AMA get it right?. Missouri Med, 2014; 111: 104.
[92] Furlong A. Scientists Find New Genetic Triggers for Obesity Risk. Bloomberg.com. Accessed 13 April 2024. Available at:[Web]
[93] Gilbert S. The Genetics of Obesity: A New Narrative or the Same Old Story?. Accessed 13 April 2024. Available at:[Web]
[94] Ayers JW, Hofstetter CR, Irvin VL et al. Can religion help prevent obesity? Religious messages and the prevalence of being overweight or obese among Korean women in California. J Sci Stud Relig, 2010; 49: 536-549.[DOI]
[95] Upenieks L, Hill TD, Ford-Robertson J. Religion and Pandemic Weight Gain: A Refuge from the Storm?. J Psychol Theol, 2023; 51: 392-411.[DOI]
[96] Jo AM, Maxwell AE, Yang B et al. Conducting health research in Korean American churches: Perspectives from church leaders. J Commun Health, 2010; 35: 156-164.[DOI]
[97] Dietz WH, Benken DE, Hunter AS. Public health law and the prevention and control of obesity. Milbank Q, 2009; 87: 215-227.[DOI]
[98] Sacks G, Swinburn B, Lawrence M. Obesity Policy Action framework and analysis grids for a comprehensive policy approach to reducing obesity. Obes Rev, 2009; 10: 76-86.[DOI]
[99] Long MW, Gortmaker SL, Ward ZJ et al. Cost effectiveness of a sugar-sweetened beverage excise tax in the U.S. Am J Prev Med, 2015; 49: 112-23.[DOI]
[100] An R. Effectiveness of subsidies in promoting healthy food purchases and consumption: a review of field experiments. Public Health Nutr, 2013; 16: 1215-1228.[DOI]
[101] Broeks MJ, Biesbroek S, Over EAB et al. A social cost-benefit analysis of meat taxation and a fruit and vegetables subsidy for a healthy and sustainable food consumption in the Netherlands. BMC public health, 2020; 20: 1-12.[DOI]
[102] Reporter LBE. Catholic schools' test scores often better than public schools: C.D. Howe report. Accessed 10 October 2024. Available at:[Web]
[103] Pankowski L. Body-Positive Companies for People With Obesity. Accessed 14 April 2024. Available at:[Web]
[104] Allison DB, Zannolli R, Narayan KM. The direct health care costs of obesity in the United States. Am J Public Health, 1999; 89: 1194-1199.[DOI]
Copyright © 2024 The Author(s). This open-access article is licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, sharing, adaptation, distribution, and reproduction in any medium, provided the original work is properly cited.


