The Maternal Health Literacy of South Asian Newcomer Mothers and Canadian-born Mothers: A Narrative Inquiry Using Propositional Analysis
Dahlia Khajeei1, Hannah T. Neufeld1, Lorie Donelle2, Samantha B. Meyer1, Elena Neiterman1, Jabeen Fayyaz3, Megan Mack4
1Faculty of Health, School of Public Health Sciences, University of Waterloo, Waterloo, Ontario, Canada
2College of Nursing, University of South Carolina, Columbia, South Carolina, USA
3Massachusetts General Hospital Institute of Health Professions, Harvard University, Boston, Massachusetts, USA
4Health Science, Thompson Rivers University, Kamloops, British Columbia, Canada
*Correspondence to: Dahlia Khajeei, Faculty of Health, School of Public Health Sciences (SPHS), University of Waterloo, 200 University Avenue, Waterloo, N2L3G1, Ontario, Canada; Email: dkhajeei@uwaterloo.ca
DOI: 10.53964/jia.2024003
Abstract
Objective: First, this comparative analysis of comprehension aimed to guide care and assist with health education research and practice as indicated in mothers stories of learning. Second, this research aimed to determine the comprehension processes of participants by comparing and characterizing the quantity and quality of the concepts’ mothers use in their narratives. Maternal health literacy (MHL) allows mothers to apply health information across all healthcare settings to make decisions about their health. Comprehension and reasoning are essential MHL skills for applying health advice.
Methods: Using narrative inquiry methodology and transformative learning theory as the lens, the comprehension processes of English-speaking South Asian Newcomer Mothers (SANMs) (n=7) were compared with those of English-speaking Canadian-born mothers (n=7). Through semi-structured interviews, the mothers discussed their comprehension of ultrasound examination preparation, health risk information, and shared decision making. Themes were identified using inductive thematic analysis, with two reviewers identifying latent themes concerning situational and sociocultural MHL practices. Then, excerpts were explicated using propositional analysis, which systematically identified the features of thought and behavior at an individual level, to identify semantic features of discourse comprehension as a form of methodological triangulation. Next, the narratives were quantified to identify latent patterns of comprehension processes, conceptual knowledge, and semantic discourse features.
Results: The key findings indicated that mothers demonstrate MHL through reifying, posturing, and volition, and that all mothers engage in knowledge-building activities and experiential learning in their communities to learn relationally from each other.
Conclusion: Ultimately, MHL empowers all mothers to become more engaged during medical appointments and in health decision making.
Keywords: maternal health literacy, narrative inquiry, propositional analysis, spoken language processing, South Asian, Canada
Canada is composed of over 250 different ethnicities who speak approximately 200 languages[1]. Between 2016 and 2021, 1.3 million newcomers settled in Canada and 62% of whom were born in Asia[2]. By 2031, approximately 25-28% of the Canadian population will comprise of newcomers[3], with more than 80% of the influx attributed to migration[4]. Newcomers may have high health literacy (HL), but those with poor official language proficiency may be unable to interpret health information. HL refers to, “the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand, and use information in ways which promote and maintain health (p. 357)[5]”. Similarly, health numeracy (HN) indicates the ability to perform numerical operations in healthcare settings to make health decisions[6]. Alarmingly, “88 adult women are considered literate for every 100 adult men globally (p. 17),” with fewer who successfully manage their health[7]. Newcomer women may be unable to comprehend health information because of challenges with multi-lingual practice[8]. The research evidence illustrated literacy and HL gaps affecting healthcare experience. For example: (1) words may not translate directly between different languages[9,10]; (2) low language competencies may affect access and use of healthcare services[11,12]; and (3) poor comprehension may affect participation in medical diagnostics[13,14]. Ultimately, literacy and HL are crucial for historically disadvantaged groups, such as newcomer women, to help them understand the systemic reasons behind their health status in order to promote their health[15]. Furthermore, newcomer women experience barriers to learning related to confidence, motivation, and self-efficacy[16].
Providing mothers with opportunities to build skills and confidence could enhance their maternal health literacy (MHL)[17]. MHL refers to the cognitive and social skills that build women’s confidence in comprehending health information, and allows mothers to access healthcare services, engage in appointments, and follow medical guidance[17,19]. The empirical literature suggests that MHL and HN conceptualizations may be organized by the themes of sociocultural demographics, self-efficacy, communication, information seeking and operationalization, health status, and reasoning[18]. Health education can help South Asian women develop MHL in the aforementioned areas, however, only 60% of South Asian women received health education in their home countries[20]. South Asian was defined as, “any person who reports an ethnicity associated with the southern part of Asia or who self-identifies as part of the South Asian visible minority group (p. 21)[21]”. South Asian newcomer mothers (SANMs) who migrate to Canada experience a variety of stress-inducing factors such as cultural change, inadequate health insurance coverage, loss of social support systems, economic uncertainty, low social status, and barriers in access to healthcare[22]. Thus, developing MHL through antenatal health education enhances knowledge, skills, and competencies for a successful parenting experience[17]. Interventions to help SANMs with health decision making in healthcare settings may target health knowledge, self-efficacy and motivation, peer and social group influence, and even provide opportunities for MHL practice in the community[15].
Central to the present study is Farrell et al.’s[23] research which highlighted the comprehension of prenatal diagnostics may be poor because mothers lack knowledge of its advantages and disadvantages. Mothers are also uniformed that ultrasound has a non-zero false positive rate, suggesting a misunderstanding of its capabilities, safety, and purpose[24]. In North America, mothers use ultrasound to make prenatal health decisions during the first eight weeks of pregnancy or during a routine ultrasound appointment prior to 20 weeks[25-27]. Ultrasound plays into a fetal culture which is subject to the discourse of medical observation[28]. Fetal culture refers to, “the effect of routine ultrasound imaging of the fetus not only on the larger cultural climate of reproductive politics, but also on the experience and consciousness of pregnant women” (p. 265)[29]. For example, ultrasound is an opportunity to rehearse parental roles[30], practice surveillance in determining family membership[31], demonstrate pregnancy management when dealing with anxiety[32], and experience the psychological reward of parental bonding[24]. Fetal culture incorporates the mothers’ behaviors and customs and is based on the experience of her body in healthcare settings[28]. Yet investigations of pregnant mothers’ perceptions and experiences of ultrasound suggest a conflict between impending health decisions and the available choices[26] - a conflict that can be distressing if diagnostics are not clearly understood due to a lack of health education[33].
This research examines the relationship among language, language competencies, and comprehension by exploring the sociocultural linguistic significance for SANMs and Canadian-born mothers. In doing so, health information access was addressed by exploring learning processes at an individual level pertaining to comprehension of ultrasound examination preparation, health risk information, and shared decision making. Ultrasound was selected because mothers, “feel”, “see”, “hear” and “connect” with their babies for the first time during an ultrasound. The research questions guiding this narrative inquiry are as follows: (1) What are the stories of ultrasound shared by English-speaking SANMs and English-speaking Canadian-born mothers? and (2) How do the sample of mothers comprehend ultrasound examination preparation, health risk information, and shared decision making? The findings of this research are intended for public health practitioners, health educators, and healthcare providers who seek information on how to assist mothers with learning.
2 METHODS
Narrative inquiry provides researchers with the opportunity to explore mothers’ stories through sociocultural linguistic narratives indicative of their motherhood journey, in settings reflective of culture and norms, of which stories represent an accurate depiction of world events[34,35]. The assumptions of narrative inquiry are stories contain actors and a plot that is resolved in a series of events occurring in chronological order[36]. This research applied the constructivist worldview originally described by Berger and Luckmann in 1966 to understand what and how stories of learning are co-constructed between the researchers and participating mothers based on their perceptions and experiences[37,38].
The mothers’ narratives were also explicated using propositional analysis, revealing comprehension discourse, to illustrate a method of spoken language processing (Figure 1)[39]. A “proposition” is the basic representation of units of narrative language composed of a predicate and argument[39]. According to the construction-integration theory of text comprehension, people think in terms of propositions organized in the mind as a network of concepts[40]. Questions regarding whether a proposition is true can be answered by looking at the relationships within and between semantic networks to understand individual thoughts and behaviors[39]. Thus, semantic networks represent the ‘situativity’ of a mother based on her unique perception and experience of the world[39], and reveal the causal structure used to solve problems[41]. Discourse refers to the politics of language and the way speech and thought order reality that both permit and restrain knowledge production[42]. As such, discourse analysis affords healthcare researchers with novel ways to analyze syntax and semantics in the context of social and historical situatedness[42]. Transformative learning theory was then applied as the lens for identifying whether a mother’s thinking and experiential learning were open to change, and for providing recommendations to guide care and assist with health education research and practice[43].
|
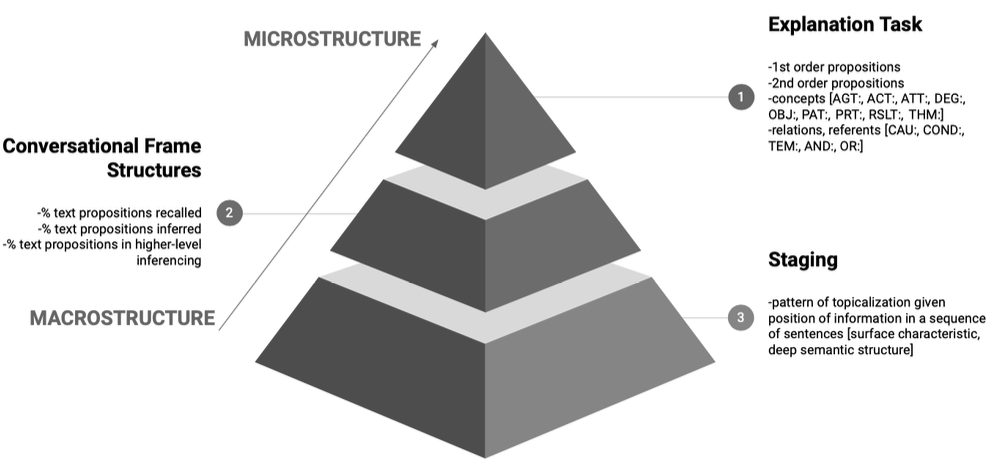
Figure 1. Semantic features of comprehension discourse.
2.1 Participant Recruitment
Prior to recruitment, the research team acquired ethics approval from the University of Waterloo Ethics Review Board (REB #43128). Information flyers were used to recruit a purposive sample of healthy (self-reported), adult (18 years of age and older), women. The research team accessed mom groups on Facebook and used snowball sampling with the assistance of community organizations to advertise the research. The community organizations included a cultural center in the Greater Toronto Area located in Ontario, Canada. Mothers were recruited from the Greater Toronto Area because of its cultural diversity[44]. A screening questionnaire was developed to determine eligibility. To be included in the study, mothers had to have had a minimum of one ultrasound during pregnancy, live in Ontario, and either be born in Canada or have migrated to Canada from South Asia. According to Statistics Canada, Asian newcomers represent the, “top source region,” of new immigrants to Canada and this trend continued in 2021 from the last 50 years (n.d.)[2]. South Asians include those who self-identify as, “East Indian”, “Pakistani” and “Sri Lankan”, which represents the largest visible minority population in Toronto according to the 2016 Toronto Population Centre Census Profile[44]. SANMs in the sample had lived in Canada anywhere from 1-40+ years. The term “newcomer” was defined according to Statistics Canada’s[45] definition of a person who is a landed immigrant or permanent resident, and who has the right to live in Canada. The SANMs were native Punjabi, Hindi, Urdu, Tamil, or Gujarati speakers. The sample of Canadian-born mothers were of any racial or cultural background. All mothers were informed that their participation was voluntary and were compensated with a $10 gift card.
2.2 Data Collection
Virtual semi-structured interviews ranging from 45 to 60 minutes were held with fourteen mothers, during the fall of 2021, which included seven English-speaking SANMs and seven English-speaking Canadian-born mothers. Sample size was based on prior research that collected narratives and analyzed verbal protocols[38,39]. A one-page interview guide (Table 1) was provided to mothers to reduce feelings of stress among those who may have been sensitive to discussing their MHL[46]. Interviews were audio-recorded and transcribed verbatim. The narratives reflected an explanation task, as mothers discussed or described what they knew about ultrasound examination preparation, health risk information, and shared decision making[47]. Doing so afforded researchers an understanding of comprehension processes, the type of conceptual knowledge a mother had, and what she may gain from learning[48]. The process of member checking the mothers’ transcripts was utilized to ensure the credibility of the representation of the mothers’ experiences; for example, the transcripts were shared via email with mothers after the (1) semi-structured interviews, and (2) coding to check for meaning[38]. The interviews continued until data saturation was reached[49].
Table 1. Semi-structured Interview Questions for Narrative Inquiry
Index |
Contents |
Ultrasound Examination Preparation |
What does learning about ultrasound examination preparation help you do? |
How does learning about ultrasound examination preparation help your pregnancy? |
|
Why would you want to learn about ultrasound examination preparation? |
|
Health Risk Information |
What does learning about health risk information help you do? |
How does learning about health risk information help your pregnancy? |
|
Why would you want to learn about health risk information? |
|
Shared Decision Making |
What does learning about shared decision making help you do? |
How does learning about shared decision making help your pregnancy? |
|
Why would you want to learn about shared decision making? |
2.3 Data Analysis
Interview transcripts from the semi-structured interviews were analyzed by two different members of the research team. NVivo 12.7.0 was the data management software used to organize the data analysis. To analyze the data, the three-step method for inductive thematic analysis proposed by Braun and Clarke[50] was used, which included: (1) data familiarization and coding; (2) developing patterns from codes to themes; and (3) synthesizing and interpreting cross-cutting themes. The preliminary codes were developed based on an initial reading of the transcripts before identifying underlying themes[50]. Latent themes reflected a single dominant concept containing several similar ideas derived from an iterative process of re-engaging with the data to identify codes and organize them into a visual thematic map[50]. The inter-coder percentage agreement was 93.0%, with the acceptable threshold being 80% or more based on published reviews [50]. Next, illustrative excerpts underwent text explication using propositional analysis to identify cognitive representations. A cognitive representation is a person’s unique mental model of a situation, process, or event, reflective of thought which accurately depicts world events[39,40]. Narratives were coded by numbering them into predicate-argument strings and deductively explicating meta text according to semantic features in medicine[39]. Cognitive representations consist of concepts and relations[39]. The codes for concepts included AGT = agent, ACT = action, ATT = attribute, DEG = degree, OBJ = object, PAT = patient, PRT = part, RSLT = result, and THM = theme or feeling[39,51]. The codes for relations included (CAU: X causes Y), conditional (COND: X implies Y), temporal (TEM: X occurs before or after Y), or Boolean (AND, OR, X is in front/left of Y, X is a variety of Y) clauses[39]. The co-author (J.F.) performed expert review of the thematic analysis results and findings to enhance credibility.
To maintain the integrity of the qualitative research, several strategies were implemented to enhance credibility[38]. The authenticity of the research was ensured by using thematic analysis in conjunction with propositional analysis to enhance the meta-synthesis of key findings[38]. To remain reflexive and enhance trustworthiness, the lead author acknowledged that she is a hyphenated, Canadian-Iranian woman; such positioning affects the interpretation of this research in that she has knowledge of Western medicine, and is an “etic”[38]. Professionally, the first author has worked with children, vulnerable populations, and mothers, which provided rich insight into interpretations by knowing how different learners construct and apply information. Further enhancing the credibility of the conclusions are the: (1) discussions with the advisory team that includes a diversity of substantive theoretical and methodological knowledge; (2) status of the co-author who is a South Asian woman and physician of women’s health, that served as an external auditor to the research[38].
Within the sample of fourteen mothers, eight (57%) were 18-32 years old, and six (43%) were 33-42 years old (Table 2). The mothers were either pregnant or had one or more children at screening. All of the mothers self-identified as being married or in a domestic partnership. Mothers engaged in a variety of employment opportunities. All the mothers indicated having English language instruction in elementary, middle, and high school; accordingly, all fourteen interviews were conducted in English. Mothers maintained a healthy lifestyle (self-reported), which consisted of engaging in physical activity several times a week, eating foods low in salt, fat, and sugar, and refraining from smoking cigarettes or drinking alcohol. Four (29%) of the SANMs were born in India, and three (21%) were born in Pakistan. The majority of the SANMs had spent 1-20 years in Canada.
Table 2. Sociodemographic Characteristics of Participants (n=14)
Index |
Value |
Count (n) |
Percent (%) |
Age (years) |
18-32 |
8 |
57 |
33-42 |
6 |
43 |
|
Employment |
Full-time for wage (40 or more hours per week) |
9 |
65 |
Part-time for wage (up to 30 hours per week) |
3 |
21 |
|
Self-employed |
1 |
7 |
|
Homemaker |
1 |
7 |
|
Country of Origin for SANMs |
India |
4 |
29 |
Pakistan |
3 |
21 |
|
Time in Canada for SANMs (years) |
1-20 |
5 |
36 |
21-40+ |
2 |
14 |
Pseudonyms, age (years), countries of origin, and time in Canada (years) of the sample of SANMs and Canadian-born mothers are included in Table 3 to provide context for the results. Pseudonyms of SANMs and Canadian-born mothers were used to maintain the confidentiality of participants and do not reflect real names. After triangulating thematic analysis with propositional analysis, the key findings suggest (1) reifying, (2) posturing, and (3) volition inform MHL in healthcare settings. These key findings are presented as illustrative excerpts consistent with the results of the latent themes and explications of text segments. The key findings were explained based on a comparison of the comprehension processes of SANMs with those of Canadian-born mothers, as depicted in their respective stories of learning using ultrasound as the entry point.
Table 3. Pseudonyms of SANMs and Canadian-born Mothers
Name |
Sample (n=14) |
Age (years) |
Country of Origin |
Time in Canada (years) |
Maha |
South Asian |
33-42 |
India |
1-20 |
Fatima |
South Asian |
18-32 |
India |
1-20 |
Tara |
South Asian |
33-42 |
India |
21-40+ |
Shakira |
South Asian |
18-32 |
India |
1-20 |
Navi |
South Asian |
18-32 |
Pakistan |
1-20 |
Rand |
South Asian |
33-42 |
Pakistan |
1-20 |
Aneet |
South Asian |
33-42 |
Pakistan |
21-40+ |
Victoria |
Canadian |
18-32 |
Canada |
N/A |
Brenda |
Canadian |
18-32 |
Canada |
N/A |
Estelle |
Canadian |
18-32 |
Canada |
N/A |
Mariah |
Canadian |
33-42 |
Canada |
N/A |
Lindsey |
Canadian |
18-32 |
Canada |
N/A |
Emily |
Canadian |
33-42 |
Canada |
N/A |
Jana |
Canadian |
18-32 |
Canada |
N/A |
3.1 Reifying
In the mothers’ narratives, reifying describes how mothers make abstract knowledge and experiences concrete, through dialogue and action. The aforementioned occured when comprehending ultrasound examination preparation by drawing on their instincts and experience to build relationships (Figure 2). Reifying represents a meta-synthesis of results from thematic analysis and propositional analysis. For example, a theme in the ultrasound examination preparation comprehension of SANMs is learning to develop a ‘sense of security’ which contrasts the learning by Canadian-born mothers who become the ‘cooperative patient.’ The ‘sense of security’ theme is defined as those internal feelings of safety and protection mothers develop with their baby. The ‘cooperative patient’ theme is defined as mother’s motivation to enhance cooperation with their healthcare providers.
|
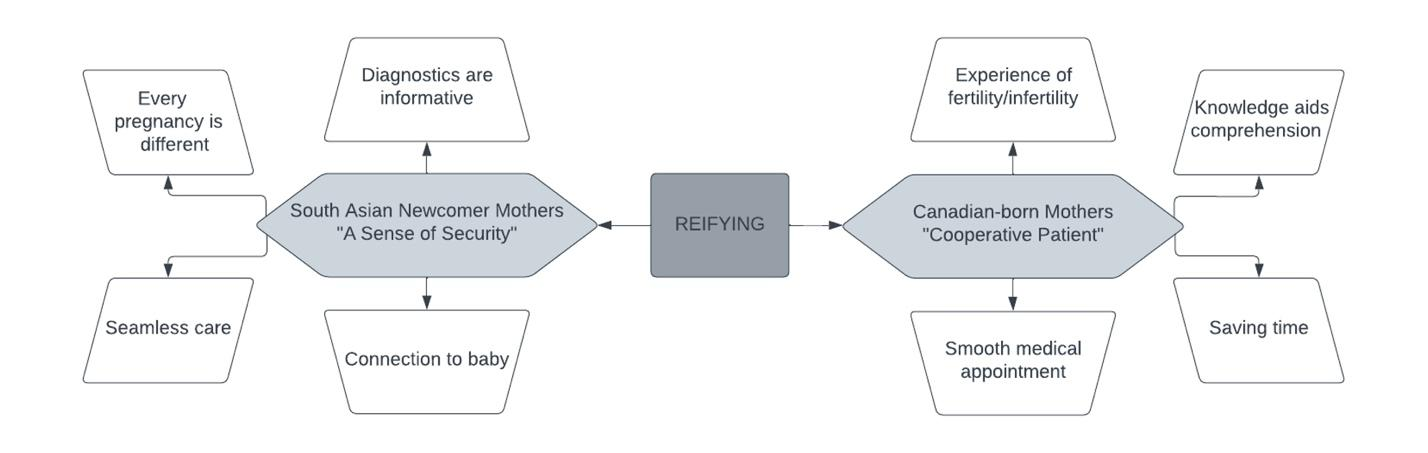
Figure 2. Themes related to the comprehension of ultrasound examination preparation.
Among the mothers, most SANMs described bonding with the baby via ultrasound in the same way as Canadian-born mothers do. However, SANMs stressed of innate sensations as they connected with the fetus in-utero which was typically absent from the Canadian-born mothers’ explanations. The data from mothers’ responses regarding how ultrasound helped the SANMs connect with the baby included Maha noting that she experienced, “excitement because I get to see my child. Not literally, but…you’ll get to see you have life inside you.” Most of the SANMs described talking to the baby and having the baby respond, which are signs of a secure mother-child bond confirmed by informative diagnostics. The responses concerning how diagnostics are informative included the topic of prenatal testing, which Rand explained, “helped me find out if my kid ha[d] any autism or genetic disorders…[putting] my mind at ease.” Feelings of reassurance to alleviate anxiety are consistent between SANMs and Canadian-born mothers. However, several SANMs discussed the motor reaction of the fetus in-utero, noting that the babies responded to the mother. Fatima noted, “[During] my ultrasounds…I have felt the heartbeat.” Here, Fatima described how, through ultrasound, sounds and physical sensations indicated the wellness of the baby in the womb. In another example, Maha stated, “when I just think about it, talk to my child internally, okay, fine, I get a yes in the form of a kick or something like some somersault”.
The propositional analysis of this excerpt identified the predicates of, ‘think’, ‘talk’ and ‘get’ as describing the perceptions and actions involved in reifying to build a ‘sense of security.’ (See Appendix 1, Text Segment 1-4) This illustrative excerpt links thinking to talking patterns with one’s baby. Thus, the SANM in this instance appears to use sensations to confirm her ‘sense of security’ through the mother-child bond.
Ultrasound examination preparation also ensured a seamless care experience between successive healthcare appointments. The data from SANMs’ responses regarding ultrasound and seamless care, for example, included Fatima’s statement that, “[Ultrasound] allows you to be set up for success.” Therefore, the SANMs built a ‘sense of security’ by turning inward to substantiate their experiences, beliefs, and health behaviors (HBs) because every pregnancy is different. The data from SANMs’ responses involving an ultrasound’s role in indicating that every pregnancy is different included Rand’s statement that an, “[Ultrasound] helps me not compare. One child can be different from the [experience] of pregnancy itself,” which made her feel more secure about her baby’s health. SANMs who had lived in Canada for 21-40+ years sought further clarification of medical directives than SANMS in Canada for 1-20 years. For example, Aneet mentioned, “I would ask for a lot of clarification…I make it a point to because I’m the one consuming this stuff.” Typically, the SANMs who had spent more time in Canada displayed more empowerment for their health outcomes and reifying was a mechanism to solidify their ‘sense of security,’ based on their prior experience with the healthcare system.
The narratives of both the SANMs and the Canadian-born mothers indicated how ultrasound gives them knowledge and reduces stress when learning to prepare for a newborn. Nevertheless, most of the Canadian-born mother’s ultrasound examination preparation comprehension was motivated by being a ‘cooperative patient’ when in communication with healthcare providers. Canadian-born mothers trusted the Canadian healthcare system and wanted to save time to ensure, “the process [went] a lot more smoothly… [by not asking] a lot of unnecessary questions to your doctor, which makes him oh so happy,” as Jana stated. Here, the Canadian-born mother displayed comprehension of medical discourses for interaction during encounters to cooperate with their healthcare providers based on their individual disposition. Victoria recounted, “making sure that I followed the instructions to make it easier on the technician to get the information they need in order to provide timely data to my doctor so that we can make the correct decisions”.
The propositional analysis of the aforementioned Canadian-born mother’s narrative identified the predicates of, ‘follow’ and ‘provide’ to describe the perceptions and actions involved in reifying to become a “cooperative patient” (See Appendix 1, Text Segment 5-9). The illustrative excerpt from Victoria’s response contained two instances of a give-and-take exchange with her healthcare provider.
According to the Canadian-born mothers’ stories about engaging with informative resources on ultrasound, they consulted their husbands and friends about what to expect from an ultrasound, which contributed to a positive experience. For instance, Lindsey stated, “My husband and I…are both people of science…we understand the literature quite well…seeing that they were published in reputable journals…we disseminate that information, and we’d discuss it with each other, and then I would discuss it with my obstetrician.” Noteworthy here is that, unlike the SANMs in the sample, the Canadian-born mothers consulted scientific journals as sources of health information on pregnancy. The SANMs preferred seeking the advice of other mothers through dialogue and engaged with print material on the Internet and in books. However, both Canadian-born mothers and SANMs used a variety of resources to learn, and both relied heavily on their healthcare providers for information.
For most of the Canadian-born mothers, learning about ultrasound was motivated by wanting to ensure normal infant development, having a stress-free medical appointment, and knowing how the procedure applied to their individual dispositions. Thus, they spoke of trust and an intrinsic motivation to learn while embodying a ‘cooperative patient’. The data from the mothers’ responses supporting the reifying of Canadian-born mothers as a ‘cooperative patient’ included the following statement by Estelle, “I have such trust in the system that [when] any medical professional says, like, ‘Go lie down on the table,’ I will do it. To me, it wasn’t really ever questioning what [the healthcare providers] were doing; it was more like what’s the information that’s going to come out of [the ultrasound]?”
Cooperation was particularly important for Canadian-born mothers who reported difficulties with fertility. The data from Canadian-born mothers’ responses regarding how ultrasound helps with the experiences of fertility included another comment by Estelle, “I did a ton of ultrasounds, ton[s] of blood work.…I got familiar with…the mechanics of getting pregnant.” While the Canadian-born mothers used reifying in the form of abstract knowledge about medical discourse to build relationships with their healthcare providers, the SANMs who experienced high-risk pregnancies substantiated their instinctual knowledge, beliefs, and experiences with greater information seeking and visuals. Aneet, for instance, who experienced placenta previa and morning sickness throughout her pregnancy, explained, “I don’t think I was given any materials.. from the hospital or the doctor.. If I still didn’t understand what they were talking about in words, I would potentially even draw it and say, is this what you mean?”
Another example of the differences in comprehension of ultrasound between the Canadian-born mothers and the SANMs was that the Canadian-born mothers could distinguish between an abdominal and a transvaginal ultrasound - an understanding largely absent in the SANMs’ stories, even after asking if they were aware of the applications of each type of ultrasound. Generally, the stories of SANMs reveal multiple instances of identifying cultural differences, which is absent from Canadian-born mothers’ stories. Specifically, Shakira observed, “[If] my doctor [and I] have the same culture, I feel more comfortable.” A stark difference between the narratives of the two groups of mothers was that the SANMs worked toward building a ‘sense of security,’ which was attributed to variances in sociocultural linguistic perception and experience, whereas the Canadian-born mothers used reifying to change HB to cooperate and adhere to medical guidance. As Estelle stated, “I now had to change some of my behaviors as a result of the ultrasound findings. It helps you change the way you behave as a pregnant person, I guess, and potentially in decisions that you need to make as a result of the outcome.”
The propositional analysis of the above excerpt identified two instances of the theme ‘behavior’ in the argument ‘change’ to describe the roles of perceptions and actions in reifying to become a ‘cooperative patient’ during learning (See Appendix 1, Text Segment 10-13). The example indicated that information acquisition and application by some of the Canadian-born mothers reflected changed HB. A ‘cooperative patient’ changed HB based on the knowledge attained from an ultrasound with the goal of improving health.
3.2 Posturing
Posturing describes how mothers adjust and adapt when comprehending health risk information to promote positive health outcomes (Figure 3). Posturing represents a meta-synthesis of results from thematic analysis and propositional analysis. A dominant theme of the SANMs’ health risk information comprehension was learning through ‘sociocultural bridges’. This theme contrasted the Canadian-born mothers’ comprehension of health risk information for ‘prioritizing prevention’. The ‘sociocultural bridges’ theme is defined as those words or actions used to connect people, places, processes, or cultures to reduce health risks. The ‘prioritizing prevention’ theme is defined as those HBs or processes which focus on prevention of sickness or disease, rather than treatment.
|
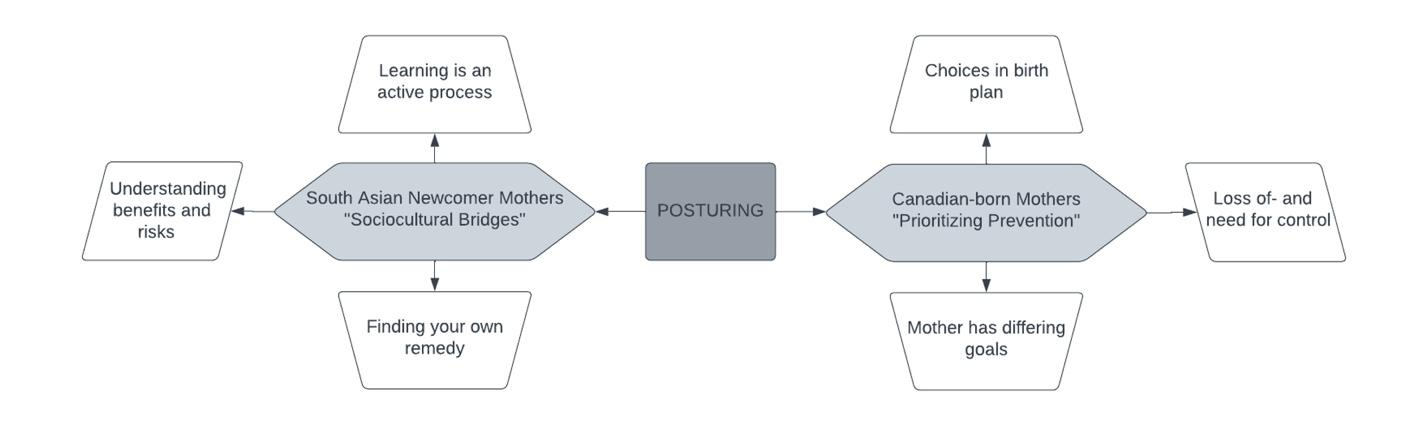
Figure 3. Themes related to the comprehension of health risk information
Most of the SANMs described the complexity of navigating sociocultural differences, such as practices of food and nutrition, traditional customs for treating ailments, and overall comprehension of motherhood. For instance, Navi explained, “I’ve not felt my doctor asked anything about it [cultural foods], but I have to tell her that I don’t eat specific meats”. In another example related to child development and the information obtained by an ultrasound, Tara shared, “The growth charts ended up needing to be personalized. My son was a premature baby. The growth charts are more tailored towards Caucasian babies, so my son never really matched up to those charts. He was not in the 90th percentile. Our culture and descent are different, and the growth charts in India might look different from what [they look] like here.”
The propositional analysis of the aforementioned excerpt identified the attribute of “different” to describe SANM’s comprehension of growth charts in Canada and reflected posturing by suggesting that a ‘sociocultural bridge’ was necessary (See Appendix 1, Text Segment 14-20). This illustrative excerpt from a SANM included one instance of numerical information involving a goal that differs from Canadian practice, thus placing mothers at health risk (by Canadian standards).
The SANMs developed ‘sociocultural bridges’ in comprehending health risk information because healthcare providers did not inquire about their cultural practices. Consequently, the responsibility shifted to the SANMs to treat their learning as an active process requiring, as Shakira recounted, they, “ask the doctor…if [our] cultural practice is true.” The SANMs’ and Canadian-born mothers’ explanations of health risk information were similar in that they both noted knowledge influences HB. For example, Rand’s explanation of the motivation behind her learning about health risk information indicated how some SANMs, “Just want to know everything about their pregnancy and want to be involved in the whole process.” Furthermore, Emily, a Canadian-born mother, stated, “You want to be in control of everything that’s going on, even though [that’s] the circle of life and that might not always go our way.” Attaining knowledge of health risk information and how health practices differ across cultures helped with health decision making for SANMs.
Some of the SANMs used their physician’s guidance to make informed decisions, which required translation into the SANMs’ customs and norms. For example, Aneet emphasized, “I don’t drink any tea and coffee, but managing the amount of caffeine that [I] have is very important.” Consistent amongst the SANMs and Canadian-born mothers is the need to do additional research on information given to them by healthcare providers regarding health risks. The SANMs also acknowledged the differences between their native sociocultural traditions and Western practices in terms of health risks. As Aneet recalled, “I don’t remember all the details, but [back home], you can start feeding your baby water at a certain age, like three months or something like that. However, in Canada, it [is] not recommended that you provide [any] other liquid than milk.”
The propositional analysis of the aforementioned excerpt indicated differences in feeding practices in alignment with the circumstances of location in the predicate (See Appendix 1, Text Segment 21-23). Posturing suggested a ‘sociocultural bridge’ was necessary to provide ‘water’ or ‘milk’ based on the location of care being India or Canada, respectively. The illustrative excerpt from the SANM included an instance of numerical information involving a goal that differs from Canadian practices that put mothers at health risk (by Canadian standards).
This excerpt highlights how healthcare provisioning with regard to health risks occurs within a complex medical discourse and sociocultural environment in which Eastern and Western practices may differ in perspectives. Consistent amongst both SANMs and Canadian-born mothers is the understanding that they are to take ownership for their health. Obtaining this understanding meant discussing the advantages and disadvantages of treatment and care with the healthcare provider to develop ‘sociocultural bridges’ for SANMs. Ultimately, SANMs held themselves accountable for their health and that of their families by doing what was necessary to attain their goals while upholding sociocultural traditions.
Conversely, for the Canadian-born mothers, comprehension of health risk information involved ‘prioritizing prevention’ rather than forming ‘sociocultural bridges’. Canadian-born mothers in the sample took prenatal courses or developed birth plans, for example. The data from the responses on how health risk information influences choices in birth plans contained the following comment by Lindsey who said, “I’d prefer a vaginal delivery over a C-section, but obviously, the health of the baby comes first”. However, some Canadian-born mothers preferred a C-section, indicating that the Canadian-born mothers considered risky pregnancy situations in advance to avoid any harm to them or their baby, thus ‘prioritizing prevention’ over medical intervention. With regards to birth plans, Mariah shared, “I learned in one of those baby delivery courses that you could, through public health, come up with what your ideal game plan [is]…whether you want an epidural or not-pre-thinking through some of those decisions before the pregnancy.”
The propositional analysis of the aforementioned excerpt identified the predicates, ‘learn’, ‘plan’, and ‘pre-think’ as describing posturing (See Appendix 1, Text Segment 24-27). Furthermore, the argument contained the action of ‘baby delivery course’ as Canadian-born mothers ‘prioritized prevention’ through formal instruction.
For the Canadian-born mothers, the comprehension of health risk information involved ‘prioritizing prevention’ by obtaining knowledge in the form of numerical facts or medical jargon, which was exclusive to Canadian-born mothers. The data from the responses confirmed the SANMs did not prefer medical intervention; for instance, Shakira explained, “If we can avoid or if we [can] have another procedure, which might have less risk, then I can go for that.” Instead, the SANMs focused on a basic comprehension of medical processes. Canadian-born mothers engaged in conversations to discuss lifestyle, family history, risky behaviors, physical examinations, and other diagnostics to maintain control or regain control when lost. Consistent amongst both SANMs and Canadian-born mothers is that pregnancy is full of surprises. The data from the Canadian-born mothers’ responses on how health risk information influences a loss of and need for control included Emily’s recollection, “I actually ended up having a natural labor, but medicated delivery. I got to 10cm on my own without the epidural....[Labor] was a matter of 2-3 hours for me”. The Canadian-born mothers in the sample spoke of nuances in pregnancy, such as knowing the risk ratio for the sandal gap, articulating the pathophysiology of Pitocin, and discussing interventions for preventing gestational diabetes. For example, Lindsey knew that, “a larger gap between the big toe and the second toe…could potentially indicate down syndrome.” Canadian-born mothers showed knowledge of how to prevent common pregnancy risks and appeared well-versed in providing the number of gestational weeks in which interventions would likely occur. For instance, Victoria explained, “Learning that I should not be having more than 200mg of caffeine a day means that my normal five-cups-a-day habit had to be changed down to one”.
The propositional analysis of the aforementioned excerpt identified the role of perceptions and actions, via the predicates of, “learn”, “change” and “habit” to describe how the Canadian-born mothers ‘prioritized prevention’ by posturing (See Appendix 1, Text Segment 28-29). Furthermore, the argument contained three incidences of numerical clarification illustrating HN. This Canadian-born mother’s illustrative excerpt shows how numerical information determines the corrective actions to take to prevent health risks arising from various habits.
In this case, learning about health risk information for the Canadian-born mothers involved taking health ownership, which resulted in empowerment similarly to that SANMs experienced as Fatima explained, “I understand [health risk information], and I’m doing the right things, so I’m doing my best to not harm my baby”. Nonetheless, some Canadian-born mothers may have displayed greater empowerment than the SANMs. Victoria attributed her empowerment to the slight advantage of being, “privileged [and]…highly educated”, which added to her, “extreme, sometimes excessive confidence”.
The Canadian-born mothers also engaged in ‘prioritizing prevention’ through diets and exercise regimes because they may have held different goals than the SANMs, such as maintaining a positive body image while pregnant. Consistent amongst both SANMs and Canadian-born mothers is walking as a form of physical activity while pregnant. Maintaining a positive body image could involve writing in a food diary or participating in the targeted learning of topics of interest for Canadian-born mothers. Jana shared the following advice and precautions that she took, “do not go skiing; be careful to avoid situations where you could fall...”. I am not drinking alcohol or [taking] drugs. Before I knew I was pregnant, I went in a hot tub. You are not really supposed to go in a hot tub. I also went to the dentist and had X-rays before I knew I was pregnant and, if you read, all those things are bad for you.
The propositional analysis of the aforementioned excerpt illustrates comprehension processes in two ways .(See Appendix 1, Text Segment 30-36) First, there was indirect coherence due to the elements of a text segment consistently sharing the same argument (i.e., seven incidences of ‘I’ and six incidences of AGT: mother). Second, the four instances of negation represented special arguments in which the mother processed right from wrong action when comprehending health risks.
Ultimately, the Canadian-born mothers were more likely to negotiate in favor of their goals for their pregnancy and enacted knowledge of HN practices in comparison to the SANMs, but both were open to learning from healthcare providers when considering health risk information. In order to comprehend health risk information, SANMs learned through ‘sociocultural bridges’ by drawing connections between people, places, processes, or cultures whereas Canadian-born mothers ‘prioritized prevention’ by turning to medical treatment and intervention as a last resort.
3.3 Volition
Volition, which describes how mothers act with free-will and empowerment when making decisions, occurs after conscious deliberation (Figure 4). Volition represents a meta-synthesis of results from thematic analysis and propositional analysis. A dominant theme of decision making by SANMs was learning through ‘functional inquiry’. The ‘functional inquiry’ theme was defined as the conversational processes mothers undertook to comprehend medical directives to inform action. With regards to decision making, Aneet shared, “[informed decision making] helps you figure out and make your own decisions based on the information you have.”
|
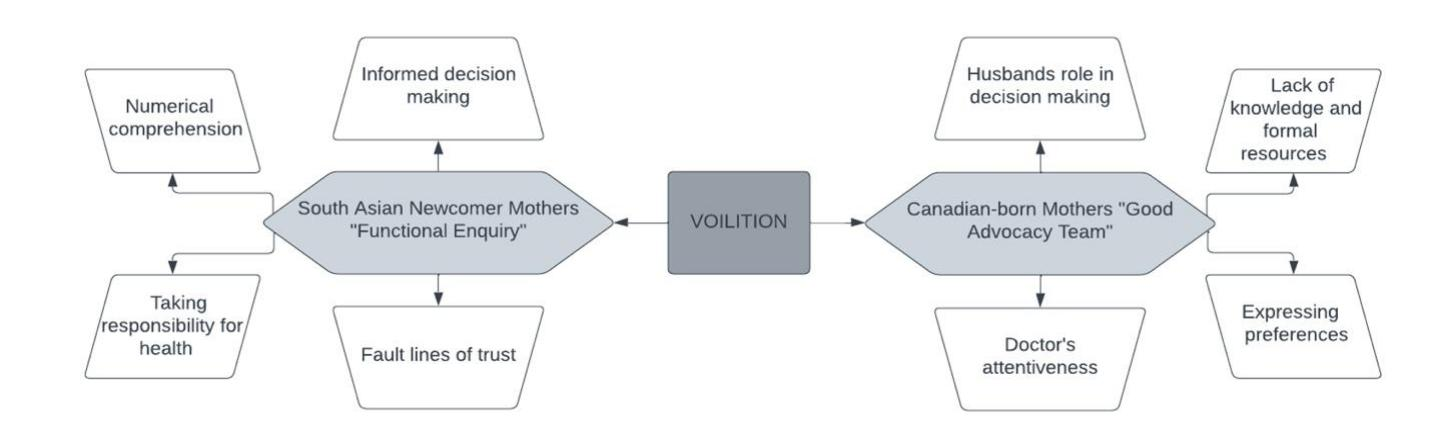
Figure 4. Themes related to the comprehension of shared decision making.
In contrast, shared decision making for the Canadian-born mothers included the development of a ‘good advocacy team.’ The ‘good advocacy team’ was defined as a cohesive unit working together to achieve shared health goals. Consistent amongst both SANMs and Canadian-born mothers is learning to clarify misconceptions. The SANMs’ ‘functional inquiry’ took the form of asking questions to advance their options because these mothers wanted to know what would happen next in their pregnancy and act accordingly. For instance, Aneet described, “getting that clarity from the prescribing doctor is extremely important”. I do not care if I have to ask it 30 times, but I need to know…[is] it one tablet or is one dose [taking] two tablets?
The propositional analysis of this excerpt used the predicates, ‘get’, ‘ask’ and ‘know’ to describe perceptions and actions in volition when displaying ‘functional inquiry’ (See Appendix 1, Text Segment 37-39). Noteworthy were Text Segments 39.2 and 39.3, in which Aneet consciously deliberated the meaning of one dose through informed decision making rather than shared decision making.
‘Functional inquiry’ suggests some of the SANMs participated in decision making to understand the consequences of their HB and to take responsibility for their health - thus, practicing MHL actively. For example, Maha stated, “whenever my doctor is telling me anything regarding some exam…I usually write down everything…so that I can easily remember.” Consistent amongst both SANMs and Canadian-born mothers is the experience of patient-directed care during encounters with their healthcare providers. However, the SANMs typically sought greater clarification to ensure they clearly understood health directions. Fatima asked the following questions, “if…we have to do [a] C-section…I asked him, when does that happen? Can you guys give me a date? What do I need to do to make sure…my placenta is still there, or is it moving up?”
The propositional analysis of the aforementioned excerpt found three instances of inadequate knowledge and comprehension when exhibiting volition during ‘functional inquiry’ (See Appendix 1, Text Segment 40-42). First, the argument string suggested that a C-section is associated with a pre-established date. Second, the placenta is not contained within the womb. Third, the mother cannot move the placenta up or down, but the opposite was stated in Text Segments 42.1-42.3. Thus, this SANM participated in informed decision making to clarify her actions.
Unlike the SANMs who engaged with informed decision making, Canadian-born mothers practiced shared decision making. Some of the Canadian-born mothers viewed shared decision making as an opportunity to develop a ‘good advocacy team’ comprising them and their husband or partner, family members, and healthcare providers. The ‘good advocacy team’ is accountable to one another by following through on medical recommendations and, in return, receiving the physician’s attention during encounters. For example, Estelle noted, “If the [physician] says, ‘This is what we have to do,’ I want them to respond to my question of ‘Well, what is the alternative?’ and not shut that down.” Both SANMs and Canadian-born mothers developed trust with their healthcare providers. The Canadian-born mothers valued emotional intelligence, empathy, and sympathy during shared decision making with the ‘good advocacy team’ as they worked together to attain the same goals. The ‘good advocacy team’ also helped Canadian-born mothers overcome the feelings of apprehension that come with pregnancy. As Brenda recalled, “I have been really happy with the care I have received from the midwives because I [found] them to be just really approachable.”
The Canadian-born mothers also displayed empowerment in expressing preferences and changing healthcare providers to establish a ‘good advocacy team’. Brenda explained, “Just being able to voice my concerns…allows me to express how I want my birthing experience.” Empowerment was crucial for some of the Canadian-born mothers to participate in self-determination during pregnancy, particularly when knowledge and resources were lacking. Empowerment also requires awareness and motivation. Jana recounted. Then I met with her [my attending] the next week and she was like.
“I saw you requested I call you. I just did not. I [was] not impressed, so I switched doctors…I think it was just a bad fit.” The propositional analysis of the aforementioned excerpt used the predicates, “impress” and “switch” to describe perceptions and actions in volition when developing a ‘good advocacy team’ (See Appendix 1, Text Segment 43-46). The end goal referred to the free-will the Canadian-born mother attained, evidenced by identifying a “bad fit” with her personal preferences.
In summary, the Canadian-born mothers formed a ‘good advocacy team’ by ensuring that their healthcare providers prioritized their goals through shared decision making. This contrasts SANMs who engaged in ‘functional inquiry’ through informed decision making in order to attain information to determine what actions to take.
This narrative inquiry explored mothers’ perceptions of, and experiences with, ultrasound as reflected through their stories of learning. It aimed to illustrate the comprehension processes of a sample of SANMs and Canadian-born mothers who practice MHL through methods of information analysis. The objective was to apply transformative learning theory to identify if a mother’s thinking and experiential learning were open to change, and to apply the construction-integration theory of text comprehension to determine participant discourse comprehension. Thus, the research did not intend to generalize about absolute differences, but explore comprehension processes of MHL in two samples. There is no relationship among the three key findings, as this is an exploratory study of narratives shared by mothers. The objective of the research was to listen to the stories of SANMs and the Canadian-born mothers in order to determine the comprehension processes of mothers, by comparing and characterizing themes, and quantifying and qualifying the concepts’ mothers use in their narratives. Thematic analysis was conducted in conjunction with propositional analysis to attain insights to contribute to health education research and practice. The key findings indicated that mothers demonstrated MHL through (1) reifying, (2) posturing, and (3) volition. This discussion considers how the key findings reflected the meta-synthesis of SANMs’ and Canadian-born mothers’ stories of learning.
Reifying described a mother’s use of abstract knowledge and experience to draw on instincts to build relationships. Reifying is defined as the MHL processes used when sensations, instincts, and intuition inform behaviors between two or more persons. Reifying is similar to cognitive embodiment, which refers to how a person’s body in everyday arenas involves situated thinking reflective of inputs from their environment[52]. Reifying changes the interactions of thinking and behavior with available tools in the environment and the proprioception of the body to impact MHL practices[52]. Reifying is made apparent through the ‘sense of security’ theme of SANMs. Reifying was illustrated by all mothers who used innate instincts (i.e., intuition and senses), knowledge (i.e., medical procedures), and experience (i.e., health decision making) during encounters. Innate instincts informed cognitive embodiment reflected in SANMs’ stories of what they thought and felt in relation to their baby or child. As a mother moved through the world, these thoughts and feelings were given life by recurring patterns in proprioception[52]. As the propositional analysis of the ‘sense of security’ theme revealed, SANMs in the sample embodied the mother-child bond via the language predicates, ‘think’ and ‘talk’ for example, of which emotions and experience give an embodied impression[53]. Health education research and practice in maternal care could provide SANMs with information on beliefs concerning mother and child safety and security in healthcare. However, noteworthy is newcomer mothers may experience barriers accessing maternal care in Canada, which is influenced by cultural competency of healthcare providers[54, 55].
Reifying was also present in the stories of the Canadian-born mothers in the ‘cooperative patient’ theme as thinking informs behavior[52]. Propositional analysis concerning the ‘cooperative patient’ theme indicated that Canadian-born mothers described the healthcare provider relationship via the language predicates, ‘follow’ and ‘provide’. Accordingly, health education research and practice in maternal care could deliver information regarding mutual beneficence between healthcare providers and mothers, for Canadian-born mothers[56] in alignment with being a ‘cooperative patient’, the Canadian-born mothers leveraged their comprehension of medical discourse to use to their advantage-a common practice in Western health systems[57]. According to the Public Health Agency of Canada[58], women have an average of three ultrasounds during pregnancy, with significant variations in the number of ultrasounds per mother, depending on their geographic location. The frequency of ultrasound may relate to the non-medical use of ultrasounds for family entertainment[59, 60]. Reifying among the Canadian-born mothers was illustrated through learning stories related to ultrasound examination to enhance relationships and as a technological tool to clarify individual disposition. In sum, ultrasound examination comprehension represented the instincts and perception, which influenced all mothers’ efforts to develop relationships and connect language and the body to the world.
Posturing describes a mother’s adjustment to health risk information to promote positive health outcomes. Similar to Kintsch’s[39] research on comprehension and cognitive representations, posturing reflects the logical structure of thinking, and comprises propositions connected by algebraic, logical, and causal relationships[39]. The aforementioned play a role in orientating and pooling[61], and adjusting and reframing[62] knowledge in informational rich environments. Posturing emphasizes a mother’s linguistic and numerical competencies as they relate to her beliefs, medical discourse, and semantic structures organized in a hierarchal, semantic net. South Asian women experience sociocultural challenges requiring the cultural transmission and negotiation at points of contestation between differing value systems[63]. The propositional analysis involving the ‘sociocultural bridges’ theme revealed some SANMs described Western healthcare conventions using the language attribute ‘different’. Thus, health education research and practice in maternal care should deliver health risk information regarding norms and customs in Western healthcare for SANMs[55]. To promote positive health outcomes and avoid health risks, MHL campaigns on health risk information should focus on SANMs and their husbands (or mothers and mothers-in-law) due to the belief in patriarchal South Asian culture that maternal health should not be discussed outside of the household[15].
The Canadian-born mothers in the sample actively pursued pregnancy goals by ‘prioritizing prevention’ via the application of logic rules to adjust to health risk information. In Canada, mothers who frequent prenatal care in the first trimester experience maternal health benefits by addressing problematic lifestyle behaviors and by detecting, monitoring, and treating pre-existing conditions[58,64]. In regards to health risks, there are differences across Canadian-born mothers of varying sociocultural demographics who experience prenatal care; for example, teenage mothers, mothers without a high school diploma, and mothers of low socioeconomic status are likelier to begin prenatal care in the second trimester - indicating barriers to ‘prioritizing prevention’[58]. Consequently, posturing may be ineffective without basic scientific knowledge, comprehension of cause-and-effect relationships, and an awareness of robust symbol systems of logic reflecting advanced information processing[39]. As the propositional analysis revealed in the ‘prioritizing prevention’ theme for our Canadian-born mother, the predicates, ‘pre-think’ ‘change’ and ‘habit’ were used. Thus, health education research and practice in maternal care could deliver information on emerging trends in prenatal and postnatal healthcare to Canadian-born mothers[65]. Ultimately, for all mothers in the sample the comprehension of health risk information was supported by health education to enhance maternal knowledge and confidence.
Volition describes a mother’s free-will and empowerment in shared decision making and entails the conscious deliberation of health information. A mother shows volition by choosing to participate in an action demonstrating that she is in charge and in control. As indicated in the ‘functional inquiry’ theme, the key finding of volition in the learning stories of the SANMs showed that mothers participated in informed decision making, rather than shared decision making. As South Asian womens’ roles in shared decision making are historically considered passive and private, SANMs may struggle with the empowerment that the Western health system provides[15]. The propositional analysis relating to the ‘functional inquiry’ theme revealed the SANMs in the sample showed conscious deliberation via the language predicates, ‘ask’ and ‘know’ indicative of informed decision making, rather than shared decision making. Thus, health education research and practice in maternal care for SANMs should deliver information on basic reproductive knowledge using infographics, numbers, and prose. Nevertheless, the historical sociocultural norms of familial permission in South Asia serve as a reminder for healthcare providers to inform these mothers of their medical options in order to help them feel empowered[15].
In contrast, the Canadian-born mothers were empowered and actively involved in their healthcare experiences forming a ‘good advocacy team’. The key finding of volition shown in their learning stories suggested that the Canadian-born mothers engaged with their friends, spouses, and healthcare providers, and were empowered to express preferences. In Canada, maternity care models favoring person-centered approaches allowing for greater self-determination could enhance healthcare quality and the perception of safety[66]. Simple steps, such as, “choice, option, and decision talk”, could also facilitate shared decision making in maternal health for all mothers (p. 1361)[67]. Propositional analysis under the ‘functional inquiry’ theme revealed that the Canadian-born mothers in the sample exercised free-will via the language predicates “switch” and “fit”. Consequently, health education research and practice in maternal care could deliver information regarding patient and family frameworks in healthcare for Canadian-born mothers[65]. To conclude, health decision making is vital to the empowerment of both SANMs and Canadian-born mothers.
This narrative inquiry has several limitations. Since purposive sampling produces results which are incapable of generalizing to a larger sociocultural group, the results are not representative of all mothers and do not account for all intersectional sociodemographic combinations. However, the research team sought rich and thick descriptions thus, achieving transferability of results[38]. Noteworthy is that mothers in one dichotomized group may have felt similar to mothers in the other dichotomized group, due to the variability within the sample. Lastly, this research focuses on adult mothers who experience live births, meaning that teenage mothers and mothers who adopt are underrepresented. Nevertheless, this research has several strengths. The research highlights mothers’ experiences as authoritative sources of knowledge about their bodies without the objectification of medical discourse[68,69]. Furthermore, using narrative inquiry as the research design and propositional analysis for methodological triangulation with thematic analysis illustrated a new application of methods for information analysis.
Transformative learning theory was applied to determine if changes to MHL were possible, as this theory postulates that mothers innately reassess their comprehension by drawing on their education, knowledge, and experience to build a new interpretation of the Western health system[43]. Transformative learning theory suggests that a mother uses her experiential learning and interpersonal skills to work with healthcare providers to critically reflect on her health decision making to make the best choice for herself and her family[43]. Accordingly, healthcare providers can identify the baseline conceptual knowledge of SANMs to provide health education by branching off these foundational points, thus helping to integrate novel health information[39]. Encouraging SANMs to engage in reading activities that reflects their circumstances could help them gain such an understanding[55,70,71]. The health education research and practice implication here is to highlight the importance of illustrating the decision pathway clearly for all mothers. By helping all mothers weigh their options given their circumstances - using infographics, mind maps, and diagrams - healthcare providers can better facilitate learning. The implication to health education research is to assess individual cognitive representations in assessments of MHL, and the implication in practice includes providing greater opportunities for all mothers to discuss their comprehension when making healthcare decisions to enhance learning.
6 CONCLUSION
The research advocates for greater transformative learning opportunities for all mothers to learn from one-another relationally. The results of the thematic analysis found SANMs developed a ‘sense of security’, built ‘sociocultural bridges’, and practiced ‘function inquiry’; whereas Canadian-born mothers embodied a ‘cooperative patient’, exemplified ‘prioritizing prevention’, and sought a ‘good advocacy team’. Ultimately, the key findings indicate that the mothers in the sample participated in the MHL activities of reifying, posturing, and volition. The implications for future research include the use of propositional analysis to systematically identify baseline conceptual knowledge for assessments of MHL as a supplement to the use of validated psychometric measures of HL and HN. In conclusion, MHL empowers socio-culturally diverse mothers to become more engaged in Canadian healthcare settings.
Our sincerest thanks go to the Calgary Board of Education, Education Matters, and Dr. E.P. Scarlett High School in Alberta, Canada, for establishing the Pourmoradi-Khajeei Educational Advancement Award for woman scholars entering Science, Technology, Engineering, and Mathematics (STEM). The Pourmoradi-Khajeei Educational Advancement Award provided opportunities for women scholars to serve as research assistants for this research. We would also like to acknowledge Punjabi Community Health Services, the Brampton Multicultural Community Centre, and the Rexdale Women’s Centre for distributing flyers to assist with participant recruitment, and sharing prior research and cultural resources pertaining to South Asian women. There are no grants or disclosures to declare.
Author Contribution
Khajeei D, Neufeld HT, Donelle L, Meyer SB and Neiterman E participated in study conception and design. Data collection and analysis was completed by Khajeei D, Neufeld HT, Donelle L, Meyer Samantha B, Neiterman E and Mack M as second coder. Interpretation of results was shared equally, with expert review by Fayyaz J. All authors reviewed the final results and approved the final version of the manuscript.
Conflicts of Interest
The author(s) received no financial support for the research, authorship, and/or publication of this article. No potential competing interest was reported by the authors.
Abbreviation List
HB, Health behavior
HL, Health literacy
HN, Health numeracy
MHL, Maternal health literacy
SANM, South Asian newcomer mother
[1] Statistics Canada. Immigration and ethnocultural diversity: Key results from the 2016 Census. The Daily, 2017: 1-8. Available at:[Web]
[2] Statistics Canada. Immigrants make up the largest share of the population in over 150 years and continue to shape who we are as Canadians. The Daily, 2022: 1-21.Available at:[Web]
[3] Malenfant É, Lebel A, Martel L. Projections of the diversity of the Canadian population 2006 to 2031. Statistics Canada, Demography Division, 2010. Available at:[Web]
[4] Statistics Canada. The Canadian immigrant labour market: Recent trends from 2006 to 2017. Accessed 24 December, 2018. Available at: [Web]
[5] Nutbeam D. Health Promotion Glossary, Health Promot Int, 1998; 13: 349-364.[DOI]
[6] Nelson W, Reyna VF, Fagerlin A et al. Clinical implications of numeracy: theory and practice. Ann Behav Med, 2008; 35: 261-274.[DOI]
[7] United Nations. Education for All: Literacy for Life. United Nations Educational, Scientific and Cultural Organization, 2005.[DOI]
[8] Im EO, Kim S, Tsai HM et al. Practical issues in multi-lingual research. Int J Nurs Stud, 2016; 54: 141-149. [DOI]
[9] Arora A, Nguyen D, Do QV et al. ‘What do these words mean?’: A qualitative approach to explore oral health literacy in Vietnamese immigrant mothers in Australia. Health Educ J, 2014; 73: 303-312.[DOI]
[10] Jacoby SD, Lucarelli M, Musse F et al. A mixed‐methods study of immigrant Somali women's health literacy and perinatal experiences in Maine. J Midwifery Wom Heal, 2015; 60: 593-603.[DOI]
[11] Carrara VI, Hogan C, De Pree C et al. Improved pregnancy outcome in refugees and migrants despite low literacy on the Thai-Burmese border: Results of three cross-sectional surveys. BMC Pregnancy Childb, 2011; 11: 1-9.[DOI]
[12] Tsai TI, Lee SYD. Health literacy as the missing link in the provision of immigrant health care: A qualitative study of Southeast Asian immigrant women in Taiwan. Int J Nurs Stud, 2016; 54: 65-74.[DOI]
[13] Eo YS, Kim JS. Associations of health belief and health literacy with Pap smear practice among Asian immigrant women. J Oncol Nurs, 2019; 42: 63-68.[DOI]
[14] Kadivar H, Kenzik KM, Dewalt DA et al. The association of English functional health literacy and the receipt of mammography among Hispanic women compared to non-Hispanic US-born white women. PLoS One, 2016; 11: e0164307.[DOI]
[15] Jafree S. The sociology of South Asian women’s health. Springer Nature: Berlin, Germany, 2020.
[16] Hills R, Kitchen S. Satisfaction with outpatient physiotherapy: A survey comparing the views of patients with acute and chronic musculoskeletal conditions. Physiother Theor Pr, 2007; 23: 21-36.[DOI]
[17] Renkert S, Nutbeam D. Opportunities to improve maternal health literacy through antenatal education: An exploratory study. Health Promot Int, 2001; 16: 381-388.[DOI]
[18] Khajeei D, Neufeld H, Donelle L et al. Maternal health literacy and health numeracy conceptualizations in public health: A scoping review. Health Soc Care Comm, 2022; 30: e3534-e3546.[DOI]
[19] Kohan S, Ghasemi S, Dodangeh M. Associations between maternal health literacy and prenatal care and pregnancy outcome. Iran J Nurs Midwife, 2007; 12:146-152.
[20] Unterhalter E. Measuring gender inequality in education in South Asia. United Nations Children's Fund, Regional Office for South Asia: Kathmandu, Nepal, 2006.[DOI]
[21] Tran K, Kaddatz J, Allard P. South Asians in Canada: Unity through diversity. Can Soc Trends, 2005; 78: 20-25.[DOI]
[22] Ahmad F, Shik A, Vanza R et al. Voices of South Asian women: Immigration and mental health. Women Health, 2005; 40: 113-130.[DOI]
[23] Farrell R, Hawkins A, Barragan D et al. Knowledge, understanding, and uptake of noninvasive prenatal testing among Latina women. Prenatal Diag, 2015; 35: 748-753.[DOI]
[24] Whynes DK. Receipt of information and women's attitudes towards ultrasound scanning during pregnancy. Ultrasound Obst Gyn, 2002; 19: 7-12.[DOI]
[25] Asplin N, Wessel H, Marions L et al. Pregnant women’s experiences, needs, and preferences regarding information about malformations detected by ultrasound scan. Sex Reprod Healthc, 2012; 3: 73-78.[DOI]
[26] Aune I, Möller A. ‘I want a choice, but I don't want to decide’-A qualitative study of pregnant women’s experiences regarding early ultrasound risk assessment for chromosomal anomalies. Midwifery, 2012; 28: 14-23.[DOI]
[27] Wick M. Mayo Clinic Guide to a Health Pregnancy. HarperCollins, 2018.
[28] Mutman M, Ocak E. Fetal Culture: Ultrasound imaging and the formation of the human. Radical Philos, 2008: 23-32.
[29] Petchesky RP. Fetal images: The power of visual culture in the politics of reproduction. In: The Medicalization of Obstetrics. Routledge: London, UK, 2021; 361-390.
[30] Roberts J, Griffiths F, Verran A. Seeing the baby, doing family: commercial ultrasound as family practice? Sociol, 2017; 51: 527-542.[DOI]
[31] Edvardsson K, Small R, Persson M et al. ‘Ultrasound is an invaluable third eye, but it can’t see everything’: A qualitative study with obstetricians in Australia. Bmc Pregnancy Childb, 2014; 14: 1-13.[DOI]
[32] Åhman A, Persson M, Edvardsson K et al. Two sides of the same coin-an interview study of Swedish obstetricians’ experiences using ultrasound in pregnancy management. Bmc Pregnancy Childb, 2015; 15: 1-10.[DOI]
[33] Furber CM, McGowan L. A qualitative study of the experiences of women who are obese and pregnant in the UK. Midwifery, 2011; 27: 437-444.[DOI]
[34] Clandinin DJ, Connelly FM. Narrative inquiry: Experience and story in qualitative research. Jossey-Bass: Hoboken ,USA, 2004.
[35] Czarniawska B. Narratives in social science research, 1st ed. SAGE Publications Ltd, 2004.[DOI]
[36] Leavy P. The Oxford handbook of qualitative research, 1st ed. Oxford University Press: Oxford, UK, 2014.
[37] Berger P, Luckmann T. The Social Construction of Reality: A Treatise in the Sociology of Knowledge. Doubleday & Company: New York, USA, 1966.
[38] Creswell J. Research design: Qualitative, quantitative, and mixed methods approaches. SAGE Publications Ltd: New York, USA, 2017.
[39] Kintsch W. Comprehension: A paradigm for cognition. Cambridge University Press: Cambridge, UK, 1998.
[40] Frederiksen C. Text comprehension in functional task domains. In: Learning to use literacy in educational settings. Ablex Publishing Corporation: New York, USA, 1988.
[41] Patel VL, Groen GJ. Knowledge based solution strategies in medical reasoning. Cogn Sci, 1986; 10: 91-116.[DOI]
[42] Cheek J. At the margins? Discourse analysis and qualitative research. Qual Health Res, 2004; 14: 1140-1150.[DOI]
[43] Mezirow J. Transformative learning theory. In: Contemporary theories of learning. Routledge: London, UK, 2018; 114-128.
[44] Statistics Canada. Census profile, 2016 census. Accessed 18 June, 2019. Available at [Web]
[45] Statistics Canada. Immigrant. Accessed 15 February, 2016. Available at [Web]
[46] Kindig D, Panzer A, Nielsen Bohlman L. Health literacy: A prescription to end confusion. National Academies Press: Washington, USA, 2004.
[47] Arocha JF, Patel VL. Methods in the study of clinical reasoning. In: Clinical Reasoning in the Health Professions, 4th ed. Elsevier: Amsterdam, The Netherlands, 2008; 147-159.
[48] Chi, M. Quantifying qualitative analyses of verbal data: A practical guide. J Learn Sci, 1997; 6: 271-315.[DOI]
[49] Patton M. Qualitative evaluation and research method, 2nd ed. SAGE Publications Ltd: New York, USA, 1990.
[50] Britton BK, Black J. Successful qualitative research: A practical guide for beginners, 1st ed. SAGE Publications Ltd: New York, USA, 2013.
[51] Bruce K. Britton, John B. Black. Understanding expository text: A theoretical and practical handbook for analyzing explanatory text, 1st ed. Routledge: London, UK, 2017.
[52] Gibbs Jr RW. Embodiment and cognitive science. Cambridge University Press: Cambridge, UK, 2005.[DOI]
[53] Ziemke T. The body of knowledge: On the role of the living body in grounding embodied cognition. Biosystems, 2016; 148: 4-11.[DOI]
[54] Ganann R, Sword W, Black M et al. Influence of maternal birthplace on postpartum health and health services use. J Immigr Minor Healt, 2012; 14: 223-229.[DOI]
[55] Higgs J, Jensen G, Loftus S et al. Clinical reasoning in the health professions, 4th ed. Elsevier: Amsterdam, The Netherlands, 2019.
[56] Salazar OAB. The meaning of humanized nursing care for those participating in it: Importance of efforts of nurses and healthcare institutions. Investigacion y educacion en enfermeria, 2016; 34: 18-28.[DOI]
[57] Song FW, West JE, Lundy L et al. Women, pregnancy, and health information online: The making of informed patients and ideal mothers. Gender Soc, 2012; 26: 773-798.[DOI]
[58] Public Health Agency of Canada (PHAC). What mothers say: The Canadian maternity experiences survey. Government of Canada, 2009.
[59] Roberts J, Griffiths FE, Verran A et al. Why do women seek ultrasound scans from commercial providers during pregnancy? Sociol Health Ill, 2015; 37: 594-609.[DOI]
[60] Stoddard R, Duffy C, Kim H et al. Effect of Race on Obstetric Ultrasound Keepsakes. Obstet Gynecol, 2023; 141: 37S-37S.[DOI]
[61] Lloyd A. Building information resilience: how do resettling refugees connect with Health information in regional landscapes-implications for health literacy. Aust Acad Res Libr, 2014; 45: 48-66.[DOI]
[62] Gele AA, Torheim LE, Pettersen KS et al. Beyond culture and language: access to diabetes preventive health services among Somali women in Norway. J Diabetes Res, 2015; 2015: 549795.[DOI]
[63] Kallivayalil D. Gender and cultural socialization in Indian immigrant families in the United States. Fem Psychol, 2004; 14: 535-559.[DOI]
[64] Heaman MI, Martens PJ, Brownell MD et al. The association of inadequate and intensive prenatal care with maternal, fetal, and infant outcomes: A population-based study in Manitoba, Canada. J Obstet Gynaecol Ca, 2019; 41: 947-959.[DOI]
[65] Ehiri J (Ed). Maternal and child health: Global challenges, programs, and policies. Springer: New York, USA, 2014.
[66] Vedam S, Stoll K, McRae DN et al. Patient-led decision making: Measuring autonomy and respect in Canadian maternity care. Patient Educ Couns, 2019; 102: 586-594.[DOI]
[67] Elwyn G, Frosch D, Thomson R et al. Shared decision making: A model for clinical practice. J Gen Intern Med, 2012; 27: 1361-1367.[DOI]
[68] Small R, Brown S, Lumley J et al. Missing voices: What women say and do about depression after childbirth. J Reprod Infant Psyc, 1994; 12: 89-103.[DOI]
[69] Lock M, Kaufert PA. Pragmatic women and body politics, 1st ed. Cambridge University Press: Cambridge, UK, 1998.
[70] Bowen JL. Educational strategies to promote clinical diagnostic reasoning. New Engl J Med, 2006; 355: 2217-2225.[DOI]
[71] Lubarsky S, Dory V, Audétat MC et al. Using script theory to cultivate illness script formation and clinical reasoning in health professions education. Can Med Educ J, 2015; 6.
Copyright © 2024 The Author(s). This open-access article is licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, sharing, adaptation, distribution, and reproduction in any medium, provided the original work is properly cited


